What Is a Stress Test? The 30-Minute Procedure That Could Predict a Heart Attack Before It Happens
The Scary Truth About Heart Disease You Can’t See Coming
Here is an uncomfortable reality that most people would rather not think about: your heart could be in serious trouble right now, and you would have absolutely no idea.
No warning. No pain. No signal.
Just the quiet, invisible progression of a condition that kills more people every year than any other disease on the planet. Heart disease does not always announce itself with dramatic chest clutching or breathlessness. More often than not, it builds in silence – slowly, methodically, and completely undetected – until the day it decides it has been ignored long enough.
That is the part nobody tells you at your annual checkup.
Most Heart Attacks Strike Without Warning
According to the American Heart Association, coronary heart disease remains the single leading cause of death in the United States, accounting for hundreds of thousands of fatalities each year. What makes this statistic especially sobering is how many of those deaths occur in people who considered themselves reasonably healthy – people who exercised occasionally, ate “well enough,” and had no history of cardiac events.
The clinical term for this is silent ischemia – a condition where the heart muscle is being deprived of oxygen-rich blood, yet the person experiencing it feels nothing at all. No chest tightness. No arm pain. No shortness of breath. Just a cardiovascular system quietly deteriorating beneath the surface while life continues as normal.
This is not a rare edge case. Research consistently shows that a significant portion of myocardial infarctions – the medical term for heart attacks – occur in individuals who had no previously diagnosed heart disease. They were not on cardiac medications. They had not been flagged as high-risk. They simply had not been tested in the right way.
And that is precisely the problem.
- Routine blood pressure checks measure force against artery walls – not whether those arteries are narrowing
- Cholesterol panels reveal lipid levels in the blood – not whether plaque has already accumulated
- Resting ECGs capture electrical activity at rest – not how the heart behaves when it is actually working hard
- Standard physical exams assess surface-level health markers – not the functional capacity of your cardiac muscle under load
Each of these tools has genuine value. But none of them alone – or even together – can fully answer the question that matters most: how does your heart actually perform when it is pushed?
The Illusion of Feeling Fine
There is a dangerous comfort in the absence of symptoms. Humans are hardwired to interpret “I feel fine” as “I am fine,” and for most health concerns, that instinct is broadly reliable. A broken bone hurts. An infection announces itself with fever. A respiratory problem makes itself known through breathlessness or coughing.
The heart, unfortunately, does not always play by those rules.
Atherosclerosis – the gradual buildup of fatty plaque inside the coronary arteries – can progress for decades without producing a single noticeable symptom. The arteries narrow slowly. The body adapts. Collateral circulation quietly compensates. And all the while, the structural integrity of the cardiovascular system is being quietly compromised.
By the time symptoms do appear – the chest discomfort, the unusual fatigue, the jaw ache that gets written off as stress – the disease has often already reached an advanced stage. In some cases, the very first symptom a person experiences is a full cardiac arrest.
This is not meant to frighten you unnecessarily. It is meant to reframe the question you should be asking your doctor.
The question is not “do I feel okay?”
The question is “how is my heart actually functioning under pressure?”
Those are two very different questions. And only one of them has the power to save your life before something goes wrong.
Why Annual Checkups Alone Are Not Enough
Most people who see their doctor annually leave feeling reassured. Blood pressure is fine. Cholesterol is within range. Resting heart rate looks good. The doctor smiles, signs off, and sends them home for another year.
And yet, cardiovascular events continue to happen to people who passed every one of those standard markers with flying colours.
The gap in the system is not negligence – it is limitation. Standard primary care appointments are designed to screen broadly across many possible health concerns. They are not designed to perform deep functional assessments of cardiac performance under physiological stress. That requires a different kind of test entirely.
It requires a test that does not just look at your heart sitting quietly at rest – but one that challenges it, pushes it, and watches what happens when it has to work.
Consider this analogy: you would never assess the true performance of a car engine by listening to it idle in a driveway. You take it on the road. You accelerate. You observe how it handles under real conditions. The engine that sounds perfectly smooth at idle may reveal a serious mechanical fault the moment it is asked to perform.
Your heart is no different.
What If a Simple 30-Minute Test Could Change Everything?
This is where the conversation shifts from sobering to genuinely empowering.
Because there is a test. A well-established, widely available, clinically proven diagnostic procedure that takes approximately 30 minutes and has the ability to reveal cardiac problems that no routine checkup can detect. A test that has been used for decades by cardiologists to peer beneath the surface of a resting heartbeat and observe what the heart is actually doing when it is asked to perform.
It is called a cardiac stress test.
And the number of lives it has saved – by catching dangerous conditions before they became fatal events – is difficult to overstate.
Imagine a 52-year-old man. No prior heart history. Slightly elevated cholesterol, well-managed with medication. Exercises occasionally. Feels tired sometimes, but he works long hours, so that makes sense. His annual physical comes back with nothing alarming. His doctor is satisfied.
Then, at his wife’s insistence, he agrees to a stress test.
Halfway through the treadmill phase, the monitoring equipment flags a significant ST-segment depression on his ECG. His blood pressure responds abnormally. The cardiologist orders an immediate follow-up angiogram. It reveals three significantly narrowed coronary arteries – a condition known as triple vessel disease, which carries a dramatically elevated risk of sudden cardiac death.
Within weeks, he undergoes bypass surgery. He is alive today.
His stress test did not just diagnose a problem. It interrupted a timeline that was moving quietly toward a catastrophic cardiac event.
That is the power of 30 minutes.
The Stakes Are Real – And Personal
Here is what makes this genuinely urgent: heart disease does not discriminate. It affects men and women. It affects athletes and sedentary individuals. It strikes people in their forties as readily as their seventies. And in a world where most people wait for symptoms before seeking deeper cardiac evaluation, the gap between “feeling fine” and “in serious danger” is often wider than anyone realises.
The good news – and there is genuinely good news here – is that when caught early, the vast majority of serious cardiac conditions are treatable, manageable, and survivable. The entire field of preventive cardiology is built on a single foundational truth: intervention before a cardiac event produces dramatically better outcomes than intervention after one.
A stress test is one of the most powerful tools available to make that early detection possible.
Frequently Asked Questions – Introduction
Now that you understand why the stakes are so high – and why routine checkups, as valuable as they are, simply cannot tell the whole story – the next logical question is an obvious one:
What exactly is a stress test, how does it work, and what actually happens during those 30 minutes?
In the next section, we break it all down in plain English – from the moment you walk into the testing room to the step-by-step process your cardiologist follows, the different types of stress tests available, and the specific equipment used to monitor every beat of your heart under pressure.
What Is a Stress Test? A Plain-English Breakdown
If you have ever wondered what actually happens behind the closed doors of a cardiac testing suite, you are not alone. For many people, the words “stress test” conjure images of complicated machinery, medical jargon, and a vague sense of anxiety about what might be discovered. The reality, however, is far less intimidating – and far more fascinating – than most people expect.
A stress test is, at its core, a brilliantly simple idea wrapped in sophisticated medical science. And once you understand exactly how it works, you will wonder why more people are not asking for one.
The Simple Definition
A cardiac stress test – also referred to as an exercise stress test, a treadmill test, or an exercise tolerance test – is a diagnostic procedure that evaluates how well your heart functions when it is subjected to controlled physical exertion.
Here is the fundamental principle: your heart, like any muscle, behaves differently under load than it does at rest. At rest, even a significantly compromised cardiovascular system can appear to function normally. Blood moves. Electrical signals fire. Pressure stays within range. Everything looks acceptable on paper. But the moment you ask that same heart to pump harder – to increase its output, accelerate its rate, and deliver more oxygenated blood to working muscles – the cracks begin to show.
Problems that hide at rest are forced into the open under stress.
That single insight is the entire basis of stress testing, and it is why the procedure has remained one of cardiology’s most valuable diagnostic tools for over half a century.
It is worth being clear about the word “stress” in this context, because it causes genuine confusion. In everyday language, stress means emotional or psychological pressure – the kind that comes from deadlines, difficult relationships, or financial worry. In the context of cardiac testing, stress means physiological demand – the physical challenge placed on the heart when the body is made to work harder than its resting state. These are entirely different things, though it is worth noting that some stress tests do use medication rather than exercise to achieve that physiological demand, which we will cover shortly.
What Happens During a Stress Test – Step by Step
Understanding the process is the single most effective way to eliminate the anxiety that surrounds this procedure. Here is exactly what you can expect, from the moment you arrive to the moment you leave.
Step 1: Pre-Test Preparation – What You Need to Do Before You Arrive
Your preparation begins well before you set foot in the testing facility. Your doctor will typically provide specific instructions, which commonly include:
- Fasting for 3–4 hours before the test – a full stomach can cause nausea during exertion and may affect results
- Avoiding caffeine for 24 hours prior – caffeine elevates heart rate and can interfere with accurate readings
- Wearing comfortable, loose-fitting clothing and supportive athletic footwear suitable for walking or light jogging
- Continuing most medications as normal unless specifically told otherwise – some medications, particularly beta-blockers, may be temporarily paused as they artificially suppress heart rate response
- Avoiding heavy exercise the day before the test
- Bringing a list of all current medications to share with the testing team
On arrival, a nurse or technician will review your medical history, confirm your current medications, take a baseline blood pressure reading, and explain the procedure in detail. This is your opportunity to ask questions – and you should absolutely use it.
Step 2: Electrode Placement and Baseline Recording
Before any physical activity begins, the technician will prepare your chest for electrode attachment. This involves:
- Lightly abrading the skin in specific locations to improve electrical contact
- Attaching 10 adhesive electrodes (small sticky patches) to precise positions across your chest, shoulders, and lower torso
- Connecting those electrodes via leads to the ECG (electrocardiogram) monitoring system
- Securing a blood pressure cuff to your arm for continuous or interval monitoring throughout the test
- Clipping a pulse oximeter to your finger to track blood oxygen saturation levels
Once everything is connected, a baseline resting ECG is recorded. This gives the cardiologist a clear picture of your heart’s electrical activity at complete rest – the benchmark against which all subsequent readings will be compared. Baseline blood pressure and resting heart rate are also formally documented at this point.
This baseline phase typically takes 10 to 15 minutes and is entirely passive on your part. You simply sit or lie still while the equipment does its work.
Step 3: The Exercise Phase – Where the Real Information Is Generated
This is the phase that most people picture when they think of a stress test, and it is where the diagnostic magic happens.
You will step onto a treadmill – or, in some facilities, a stationary exercise bicycle – and begin moving at a slow, comfortable pace. The intensity increases at regular intervals using a standardised protocol. The most widely used is the Bruce Protocol, which increases both the speed and incline of the treadmill every three minutes across a series of stages.
Stage one is genuinely easy – a gentle walk on a slight incline. By stage three or four, you are moving at a brisk pace on a noticeably steep gradient. The goal is not to exhaust you for its own sake. The goal is to gradually elevate your heart rate to a target level – typically calculated as a percentage of your maximum predicted heart rate, which is roughly estimated as 220 minus your age.
Throughout this phase, the monitoring team is watching several things simultaneously:
- ECG readings – looking for any changes in the heart’s electrical pattern that suggest restricted blood flow or abnormal rhythm
- Blood pressure response – tracking whether pressure rises appropriately with exertion or behaves abnormally
- Heart rate progression – assessing how efficiently the heart accelerates and whether it reaches the target zone
- Physical symptoms – chest pain, shortness of breath, dizziness, leg fatigue, or any other reported discomfort
- Overall appearance – skin colour, sweating pattern, and signs of distress that may not show on the monitors
You are encouraged to report any symptoms you experience during the test immediately, even if they seem minor. The testing team can stop the procedure at any point if they observe something concerning or if you feel unable to continue safely.
Step 4: Peak Exertion Monitoring – The Critical Window
The period around peak exertion – when your heart rate is at or near its maximum target – is arguably the most diagnostically valuable phase of the entire test. This is when the cardiovascular system is working hardest, when blood demand from the muscles is at its highest, and when any underlying problems with coronary artery blood flow are most likely to reveal themselves through changes in the ECG trace.
The cardiologist or supervising physician watches the monitoring equipment with particular attention during this window. ST-segment changes on the ECG – specifically depression or elevation of a particular part of the electrical waveform – are one of the most important indicators of myocardial ischemia, the condition where the heart muscle is not receiving adequate blood supply during exertion.
This phase lasts only as long as necessary to gather sufficient data at peak effort – typically just a few minutes of high-intensity exercise before the cool-down begins.
Step 5: The Cool-Down and Recovery Phase
Once the target heart rate has been achieved and sufficient data collected, the treadmill speed and incline are gradually reduced, allowing your heart rate and blood pressure to return toward baseline in a controlled manner.
This recovery phase is not just a formality. Monitoring continues throughout, because certain abnormalities – particularly some types of arrhythmias and delayed blood pressure responses – only become apparent as the heart decelerates rather than during peak exertion itself. The recovery data is considered a critical part of the complete picture.
You will be monitored for a further 5 to 10 minutes after exercise ceases, seated or lying down, until your vital signs have stabilised within acceptable ranges.
Total Time – What to Expect for Your Appointment
- Preparation and baseline: 15–20 minutes
- Active exercise phase: 8–15 minutes (depending on fitness level and protocol used)
- Recovery monitoring: 10–15 minutes
- Results discussion with physician: 5–10 minutes
Total appointment time: typically 45 to 75 minutes, though the actual exercise component is often considerably shorter than patients expect.
Types of Stress Tests You Should Know About
Not all stress tests are identical. The appropriate type depends on your specific health profile, the clinical question being investigated, and what your doctor needs to see. Here is a clear breakdown of the main variants:
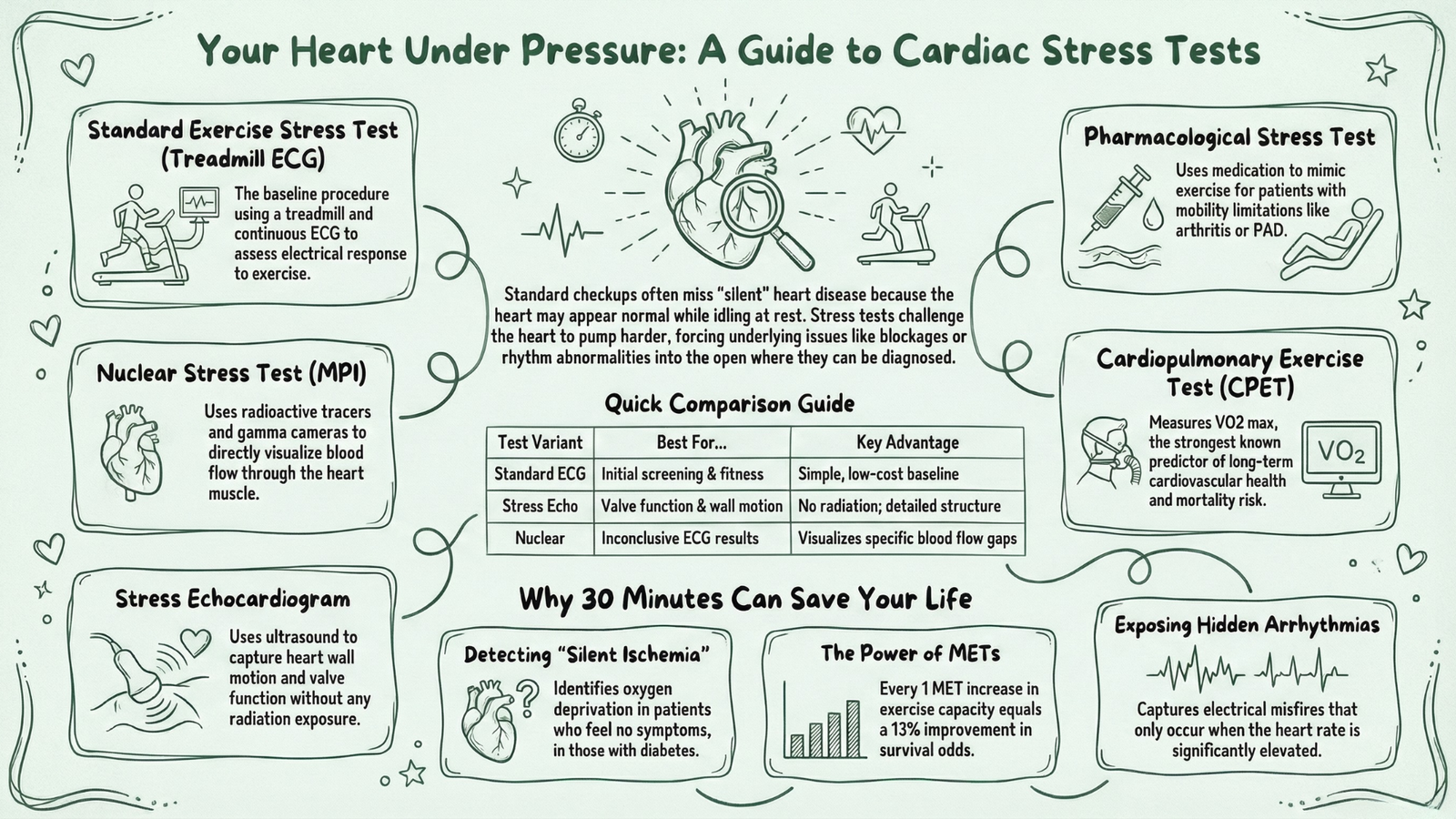
1. Standard Exercise Stress Test (Treadmill ECG Test)
This is the most common form – the baseline procedure described above. It uses a treadmill or stationary bike combined with continuous ECG monitoring to assess the heart’s electrical response to exercise.
- Best for: Initial screening for coronary artery disease, arrhythmia evaluation, fitness assessment
- Limitations: Cannot directly visualise blood flow or heart wall motion; may produce inconclusive results in certain patient groups
2. Nuclear Stress Test (Myocardial Perfusion Imaging)
This variant adds a powerful layer of visual information to the standard exercise test. A small amount of radioactive tracer – typically technetium or thallium – is injected into the bloodstream, and a specialised gamma camera captures images of blood flow through the heart muscle both at rest and during peak exertion.
- Best for: Confirming or ruling out coronary artery disease when standard ECG results are inconclusive; assessing extent of prior heart attack damage
- Key advantage: Directly visualises which areas of the heart are receiving reduced blood flow
- Consideration: Involves low-level radiation exposure and is more time-intensive
3. Stress Echocardiogram
This test combines a standard exercise stress test with ultrasound imaging of the heart. Echocardiogram images are taken immediately before and within seconds of completing exercise, capturing how the heart wall moves and contracts under load compared to at rest.
- Best for: Detecting wall motion abnormalities that indicate blocked arteries; evaluating heart valve function under stress; assessing heart failure
- Key advantage: No radiation; provides detailed structural and functional information
- Consideration: Requires rapid image acquisition immediately post-exercise – timing is critical
4. Pharmacological Stress Test
For patients who are unable to exercise adequately – due to arthritis, peripheral artery disease, severe deconditioning, or other physical limitations – medications are used to mimic the effects of exercise on the heart without requiring physical exertion.
Drugs such as adenosine, regadenoson, or dobutamine are administered intravenously to artificially increase heart rate, dilate coronary vessels, or stress the heart muscle in ways that replicate the physiological demands of exercise.
- Best for: Elderly patients, those with mobility limitations, individuals with conditions that prevent safe exercise
- Important note: This is always combined with imaging – either nuclear or echocardiographic – since ECG changes alone are less reliable with pharmacological stress
5. Cardiopulmonary Exercise Test (CPET / VO2 Max Test)
This is the most comprehensive form of stress testing, measuring not just cardiac function but the integrated performance of the heart, lungs, and musculoskeletal system simultaneously. It measures VO2 max – the maximum volume of oxygen the body can utilise during intense exercise – which is one of the strongest known predictors of long-term cardiovascular health and overall mortality risk.
- Best for: Heart failure management, pre-surgical assessment, elite athletic performance evaluation, unexplained breathlessness
- Key advantage: Provides the most complete picture of cardiorespiratory fitness available
What Equipment and Technology Is Used?
The technology behind a stress test is more sophisticated than most patients realise – and the safety infrastructure surrounding it is equally impressive.
Core monitoring equipment includes:
- 12-lead ECG system – the central diagnostic tool, capturing electrical activity from 12 different angles simultaneously to provide a three-dimensional picture of cardiac function
- Automated blood pressure monitor – tracks pressure responses continuously or at regular intervals throughout exercise and recovery
- Pulse oximeter – monitors blood oxygen saturation, flagging any drop that might indicate cardiorespiratory compromise
- Treadmill or cycle ergometer – precisely calibrated exercise equipment with programmable speed, incline, and resistance profiles
For advanced imaging variants:
- Gamma camera / SPECT scanner – used in nuclear stress testing to capture radiotracer distribution through cardiac tissue
- Echocardiography machine – high-frequency ultrasound equipment for real-time cardiac wall imaging in stress echocardiograms
- Intravenous infusion pump – for precise pharmacological agent delivery in non-exercise stress tests
Safety equipment – always present:
- Emergency crash cart with defibrillator
- Intravenous access capability
- Reversal agents for pharmacological stress medications
- Direct physician supervision throughout the procedure
This last point deserves emphasis. A cardiac stress test is never performed unsupervised. A qualified cardiologist or supervising physician is present throughout the exercise and recovery phases, with the authority and equipment to respond immediately to any adverse event.
Frequently Asked Questions – Section 2
Now that you have a thorough understanding of exactly what a stress test is, how it works from start to finish, and the range of testing options available – the next question that most people find genuinely surprising is this one:
Just how much can a 30-minute stress test actually reveal about your heart?
The answer is more than you might expect. In the next section, we walk through seven dangerous cardiac conditions that a stress test has the power to detect – conditions that often show no symptoms whatsoever until a crisis occurs – and explain precisely how the test identifies each one before it becomes a life-threatening emergency.
7 Dangerous Heart Conditions a Stress Test Can Catch Before a Crisis
Most people assume that feeling healthy means being healthy. When it comes to the heart, that assumption can be genuinely dangerous.
The cardiovascular system is capable of compensating for significant underlying damage for years – sometimes decades – before producing any symptom noticeable enough to prompt a doctor’s visit. By the time the body finally sends a distress signal, the disease process has often already reached a critical stage. This is not a flaw in the system so much as a sobering reality of how heart disease progresses.
What makes a cardiac stress test so uniquely valuable is its ability to cut through that silence. By observing how the heart performs under controlled physiological demand, it can expose conditions that a resting body has been successfully concealing – sometimes for years. The list of what it can detect is longer, and more serious, than most patients realise.
Here are seven of the most significant cardiac conditions that a stress test has the power to identify before they escalate into a life-altering – or life-ending – event.
1. Coronary Artery Disease (CAD)
Coronary artery disease is the most common form of heart disease in the world, and it is the condition that stress tests were originally designed to detect. It develops when atherosclerotic plaque – a combination of cholesterol, fat, calcium, and inflammatory cells – gradually accumulates on the inner walls of the coronary arteries, the vessels responsible for delivering oxygenated blood directly to the heart muscle.
Over time, this buildup narrows the arterial channel. The heart, at rest, may receive just enough blood to function normally – the narrowed artery is restrictive, but not restrictive enough to cause obvious problems when demand is low. The moment physical exertion increases the heart’s oxygen requirement, however, the inadequate blood supply is immediately exposed.
This is precisely what the stress test captures.
During the exercise phase:
- Heart rate and cardiac output increase significantly
- The demand for oxygenated blood to the heart muscle rises sharply
- Narrowed coronary arteries cannot meet that demand
- The resulting ischemia – oxygen deprivation of the heart muscle – produces characteristic changes in the ECG trace
- Blood pressure may respond abnormally
- The patient may begin to experience chest discomfort or unusual breathlessness
The degree of ECG change, combined with the exercise level at which it appears, gives the cardiologist a powerful indication of both the presence and severity of coronary disease. A patient who develops significant ST-segment depression early in the exercise protocol – at a low workload – is showing signs of more severe obstruction than one whose changes appear only at near-maximum exertion.
Why this matters: CAD is the leading cause of heart attacks globally. Identifying it before a myocardial infarction occurs creates an intervention window – medications, lifestyle modification, stenting, or bypass surgery – that can dramatically reduce the risk of a fatal cardiac event.
2. Abnormal Heart Rhythms (Arrhythmias)
The heart’s electrical system is a marvel of biological engineering – a precisely timed sequence of signals that coordinates the contraction of millions of cardiac muscle cells in perfect synchrony, beat after beat, for an entire lifetime. When that electrical system misfires, the result is an arrhythmia – an abnormal heart rhythm that can range from harmlessly inconvenient to acutely life-threatening.
Here is what makes stress testing particularly valuable for arrhythmia detection: many abnormal rhythms are exertion-dependent. They simply do not occur – or do not occur with diagnostic clarity – when the heart is beating slowly and calmly at rest. It is only when the heart is working hard, its rate elevated and its electrical demand high, that the instability reveals itself.
A resting ECG, taken over a period of just 10 seconds, has a very limited chance of capturing an arrhythmia that only triggers under load. A stress test, by contrast, monitors the heart’s electrical activity continuously across the full spectrum from rest to peak exertion and back again.
Arrhythmias that stress testing commonly identifies include:
- Ventricular tachycardia (VT) – a rapid, potentially dangerous rhythm originating in the lower chambers of the heart. Exercise-induced VT is a significant finding that warrants urgent further investigation
- Supraventricular tachycardia (SVT) – abnormal rapid rhythms originating above the ventricles, often triggered by elevated heart rates during exertion
- Atrial fibrillation (AF) – an irregular, chaotic rhythm in the upper chambers that increases stroke risk significantly and may only become apparent during physical activity in some patients
- Premature ventricular contractions (PVCs) – extra heartbeats originating in the ventricles that become more frequent or complex under exercise stress, potentially signalling underlying structural disease
- Heart block – a disruption in the electrical conduction pathway between the upper and lower chambers, which may worsen under exertion
Why this matters: Undiagnosed exercise-induced arrhythmias are a known cause of sudden cardiac death, particularly in younger individuals and athletes. Identifying them during a controlled, supervised stress test – rather than during an unmonitored bout of exercise – creates the opportunity for treatment before a dangerous episode occurs in an uncontrolled setting.
3. Reduced Blood Flow to the Heart (Ischemia)
Myocardial ischemia deserves its own dedicated entry, separate from the broader discussion of coronary artery disease, because it is both more nuanced and more insidious than many people realise.
Ischemia, in the cardiac context, refers specifically to an insufficient supply of oxygenated blood to the heart muscle itself. It can occur as a result of coronary artery disease – blocked or narrowed vessels – but it can also arise from coronary artery spasm, microvascular disease, or severe anaemia. Whatever the underlying cause, the consequence is the same: the heart muscle is not getting the oxygen it needs to function properly.
What makes silent ischemia particularly dangerous is embedded in its name. A substantial proportion of ischemic episodes produce no chest pain or other recognisable symptoms. The heart is being oxygen-deprived, the muscle cells are under stress, and the risk of serious damage is real – yet the patient feels nothing out of the ordinary.
This form of ischemia is particularly prevalent in people with diabetes, whose neuropathy can blunt or eliminate the pain signals that would normally accompany reduced blood flow. It is also more common in women, whose presentations of cardiac ischemia frequently differ from the classic chest-pain pattern more commonly observed in men.
How the stress test detects ischemia:
The primary marker is ST-segment change on the ECG – specifically, horizontal or downsloping depression of the ST segment by 1 millimetre or more during exercise. This change reflects altered electrical activity in ischemic heart muscle and is one of the most studied and validated findings in all of cardiology.
Additional indicators include:
- Onset of chest pain, pressure, or tightness during exercise – even if previously unreported
- Abnormal blood pressure response – failure to rise appropriately or a sudden drop
- Reduced exercise capacity disproportionate to the patient’s age and fitness level
- Recovery abnormalities – ST changes that persist or worsen after exercise ends
Why this matters: Identifying ischemia before it causes permanent heart muscle damage is one of the most impactful applications of stress testing in preventive cardiology. Treated ischemia is manageable. A myocardial infarction caused by undetected, untreated ischemia may not be.
4. Heart Valve Problems
The heart contains four valves – the mitral, aortic, tricuspid, and pulmonary valves – each responsible for ensuring that blood flows in the correct direction through the cardiac chambers. When these valves become diseased – either stiffening and narrowing (stenosis) or failing to close properly and leaking backward (regurgitation) – the heart’s efficiency is compromised.
At rest, even moderately diseased valves can maintain adequate circulation. The real problem emerges when the body demands more – during exercise, physical exertion, or emotional stress. Under these conditions, a compromised valve that seemed manageable at rest may be exposed as a much more significant obstruction to normal blood flow.
Stress echocardiography is particularly powerful for this application, as it captures real-time ultrasound images of valve function both before and immediately after exercise. This allows the cardiologist to observe directly how the valve performs under load – not just at rest – and to quantify the severity of any dysfunction with far greater accuracy than a resting echo alone.
Valve conditions commonly assessed with stress testing:
- Aortic stenosis – narrowing of the aortic valve that restricts outflow from the left ventricle. Exercise-induced symptoms or abnormal haemodynamic responses can trigger urgent reassessment even when resting measurements appear only moderate
- Mitral regurgitation – leaking of the mitral valve that worsens under exercise-induced volume load, potentially revealing a more severe degree of regurgitation than resting assessment suggested
- Mitral valve prolapse – a condition in which one or both leaflets of the mitral valve bulge backward during contraction, which may produce exercise-induced arrhythmias or regurgitation
Why this matters: Valve disease is progressive. The timing of surgical or interventional treatment – valve repair or replacement – is critically dependent on understanding how the valve performs under real physiological conditions. Stress testing provides information that resting assessments simply cannot.
5. Heart Failure Risk
Heart failure does not mean the heart has stopped. It means the heart is no longer pumping with sufficient efficiency to meet the body’s demands – a distinction that is important, but one that does little to reduce the seriousness of the condition.
Heart failure is classified broadly into two categories: heart failure with reduced ejection fraction (HFrEF), where the heart muscle is weakened and cannot contract forcefully enough, and heart failure with preserved ejection fraction (HFpEF), where the muscle contracts normally but has become stiff and cannot relax adequately to fill with blood between beats.
Both categories can be difficult to diagnose with certainty at rest, particularly in early stages. A patient may report breathlessness and fatigue with exertion – classic heart failure symptoms – yet their resting echocardiogram may appear relatively normal. This is where stress testing, particularly stress echocardiography or CPET, provides critical diagnostic clarity.
What stress testing reveals in heart failure assessment:
- Reduced exercise capacity disproportionate to age and conditioning – a sensitive early marker of cardiac pump dysfunction
- Abnormal rise in filling pressures during exercise, visible on stress echocardiography as changes in mitral inflow patterns
- Impaired cardiac output response to increasing workload – the heart fails to increase its output appropriately as exercise intensity rises
- VO2 max values below established thresholds – in CPET testing, a peak VO2 below 14 ml/kg/min is a recognised marker of severe functional limitation and informs decisions about advanced therapies
Why this matters: Early identification of heart failure – particularly the preserved ejection fraction variant, which is notoriously difficult to diagnose – allows for therapeutic intervention before significant structural remodelling occurs. In advanced heart failure, stress testing informs critical decisions about device therapy, transplant listing, and prognosis.
6. Exercise Capacity and Functional Fitness Level
This one surprises many people. A stress test does not only detect disease – it also quantifies health. And in doing so, it generates one of the most powerful independent predictors of long-term cardiovascular mortality available in clinical medicine.
Exercise capacity, measured in METs (Metabolic Equivalents of Task), represents the maximum level of physical work a person can sustain during a stress test. One MET equals the energy expenditure at complete rest. A result of 10 METs means the individual can sustain physical activity at ten times their resting metabolic rate – a reasonable level of functional fitness for a middle-aged adult.
The relationship between exercise capacity and survival is not subtle. A landmark study published in the New England Journal of Medicine found that exercise capacity was the single strongest predictor of mortality in both healthy individuals and those with cardiovascular disease – stronger than traditional risk factors including hypertension, diabetes, smoking, and obesity.
What your MET score tells your cardiologist:
- A patient who cannot achieve 5 METs during a stress test has a prognosis comparable to someone with significant known coronary disease
- Each 1 MET increase in exercise capacity is associated with approximately a 13% improvement in survival
- Low exercise capacity predicts risk independently – meaning even if every other test result is normal, a very low MET score remains a clinically significant finding
Why this matters: Exercise capacity is both a diagnostic finding and a modifiable risk factor. Unlike age or genetics, it can be improved through structured physical activity. Identifying a low MET score gives the clinical team a clear, quantifiable target for intervention.
7. Effectiveness of Current Heart Treatments
The diagnostic value of stress testing does not end at first diagnosis. For the millions of people already living with known cardiovascular disease – or who have undergone cardiac procedures – stress testing serves a critically important ongoing role in monitoring whether existing treatments are actually working.
This is an aspect of stress testing that often goes undiscussed, yet it carries enormous practical significance for patient management.
Post-procedure assessment:
Following coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI) – the procedure commonly known as stenting – a stress test can determine whether blood flow to the heart muscle has been successfully restored, and whether any new areas of ischemia have developed in the months or years since the procedure. Graft failure and in-stent restenosis are genuine concerns that may produce no symptoms in their early stages.
Medication effectiveness:
- Beta-blockers – prescribed to control heart rate and reduce cardiac workload – can be directly assessed for efficacy by observing how well they suppress heart rate during exercise. A patient whose rate spikes excessively despite medication may need dose adjustment
- Anti-anginal medications – such as nitrates or calcium channel blockers – should reduce or eliminate exercise-induced ischemia. A stress test confirms whether they are achieving this goal
- Antiarrhythmic drugs – their effectiveness in suppressing exercise-induced arrhythmias can be directly evaluated under controlled conditions
Cardiac rehabilitation monitoring:
Patients enrolled in cardiac rehabilitation programmes following a heart attack or cardiac surgery routinely undergo stress testing to safely establish exercise prescription targets and monitor functional improvement over the course of the programme.
Why this matters: Medicine without measurement is guesswork. Stress testing transforms the management of known heart disease from a passive, symptom-driven process into an active, evidence-based strategy – one where treatment decisions are informed by objective data rather than assumption.
Frequently Asked Questions – Section 3
The diagnostic reach of a stress test is clearly broader and more powerful than most people appreciate. From silent coronary disease to hidden arrhythmias, from early heart failure to the measurable fitness metric that predicts how long you are likely to live – this single 30-minute procedure generates a remarkable volume of clinically actionable information.
But knowing what a stress test can detect naturally raises a question that is equally important:
Who actually needs one – and when?
Not everyone requires a stress test, and not every situation calls for the same type. In the next section, we provide a clear, practical guide to identifying whether you are in a group that should be requesting one, the specific circumstances that typically trigger a referral, and – crucially – how to advocate for yourself if you believe a stress test is warranted but your doctor has not yet recommended it.
Do You Actually Need a Stress Test? Here’s How to Know
There is a question that sits quietly in the back of many people’s minds after reading about cardiac stress testing – a question that is equal parts practical and personal:
Is this something I actually need?
It is a fair question, and it deserves a direct answer. Not everyone requires a stress test, and ordering one indiscriminately for every adult who walks through a clinic door would be neither clinically appropriate nor cost-effective. But the opposite error – assuming that stress testing is only for people who are already sick – is far more dangerous, and far more common.
The reality is that cardiac stress testing occupies a critical space in preventive medicine that millions of people are not accessing – not because their doctors have evaluated them and determined it unnecessary, but simply because the conversation has never happened. Nobody has asked the right questions. Nobody has connected the risk factors to the available diagnostic tool.
This section is designed to change that.
High-Risk Groups Who Should Request One
Certain individuals carry a significantly elevated probability of having undetected cardiac disease – a probability high enough that proactive stress testing is not just reasonable, but genuinely important. If you fall into one or more of the following categories, a conversation with your doctor about stress testing is not an overreaction. It is informed self-advocacy.
Adults Over 40 With One or More Cardiac Risk Factors
Age alone is a meaningful risk factor for cardiovascular disease. The coronary arteries accumulate damage over time – from inflammation, oxidative stress, and the mechanical wear of decades of pulsatile blood flow. But age combined with additional modifiable risk factors creates a compounding effect that dramatically elevates the probability of significant underlying disease.
If you are over 40 and carry any of the following risk factors, a stress test discussion is warranted:
- Elevated LDL cholesterol or low HDL cholesterol
- Hypertension (blood pressure consistently above 130/80 mmHg)
- Type 2 diabetes or insulin resistance
- Overweight or obesity – particularly abdominal obesity, which is associated with visceral fat accumulation around the organs and elevated cardiovascular risk
- Physical inactivity – a sedentary lifestyle is an independent cardiac risk factor, not merely a lifestyle concern
- Chronic kidney disease – strongly associated with accelerated cardiovascular disease progression
- Inflammatory conditions – rheumatoid arthritis, lupus, and psoriasis carry elevated cardiac risk through chronic systemic inflammation
The more risk factors present, the stronger the case for proactive cardiac evaluation. A single risk factor in an otherwise healthy 42-year-old may warrant monitoring and lifestyle intervention. Three or four concurrent risk factors in a 50-year-old represent a meaningfully different clinical picture.
Smokers and Former Smokers
Cigarette smoking is one of the most aggressive accelerators of atherosclerosis known to medicine. Tobacco smoke damages the endothelial lining of blood vessels, promotes inflammatory processes, reduces HDL cholesterol, increases blood clotting tendency, and elevates blood pressure – essentially attacking the cardiovascular system through multiple simultaneous pathways.
Former smokers carry residual risk that persists for years after cessation, with cardiovascular risk not fully returning to never-smoker levels for up to 15 years following quitting. Anyone with a significant smoking history – typically defined as 10 pack-years or more – should consider proactive cardiac evaluation, including stress testing, regardless of current smoking status.
The common assumption that quitting smoking eliminates cardiovascular risk is well-intentioned but medically incomplete. The damage that accumulated during the smoking years does not simply disappear upon cessation. It needs to be assessed.
People With Diabetes
Diabetes mellitus – both Type 1 and Type 2 – deserves specific mention because of how profoundly it alters the cardiac risk landscape and, simultaneously, how effectively it masks the symptoms that would normally prompt someone to seek evaluation.
Diabetic patients are two to four times more likely to develop coronary artery disease than their non-diabetic counterparts. More importantly, the autonomic neuropathy that commonly accompanies diabetes can significantly blunt or completely eliminate the chest pain response to cardiac ischemia – meaning that diabetic patients can experience significant coronary artery obstruction and even myocardial infarction without any of the warning signals that would prompt a non-diabetic patient to seek emergency care.
This is why silent myocardial infarction – a heart attack that occurs without the patient recognising it – is disproportionately common in the diabetic population. A stress test, in this context, is not merely a precaution. For many diabetic patients, it may be the only reliable way to detect coronary disease before it causes irreversible damage.
Those With a Family History of Heart Disease
Genetics plays a meaningful role in cardiovascular risk. A family history of premature coronary artery disease – defined as a first-degree male relative (father, brother, son) diagnosed before age 55, or a first-degree female relative (mother, sister, daughter) diagnosed before age 65 – is an independent risk factor that elevates an individual’s cardiac risk regardless of their personal lifestyle choices.
This is not fatalism. Having a family history of early heart disease does not predetermine your outcome. But it does mean that your cardiovascular system may be operating with an inherited predisposition toward atherosclerosis, inflammatory response, or lipid metabolism abnormalities that warrant earlier and more proactive evaluation than the general population.
If your father had a heart attack at 52, or your sister underwent bypass surgery at 58, your cardiac evaluation timeline should not be the same as someone with no family history. A stress test earlier in life – in your late thirties or early forties – may be entirely appropriate.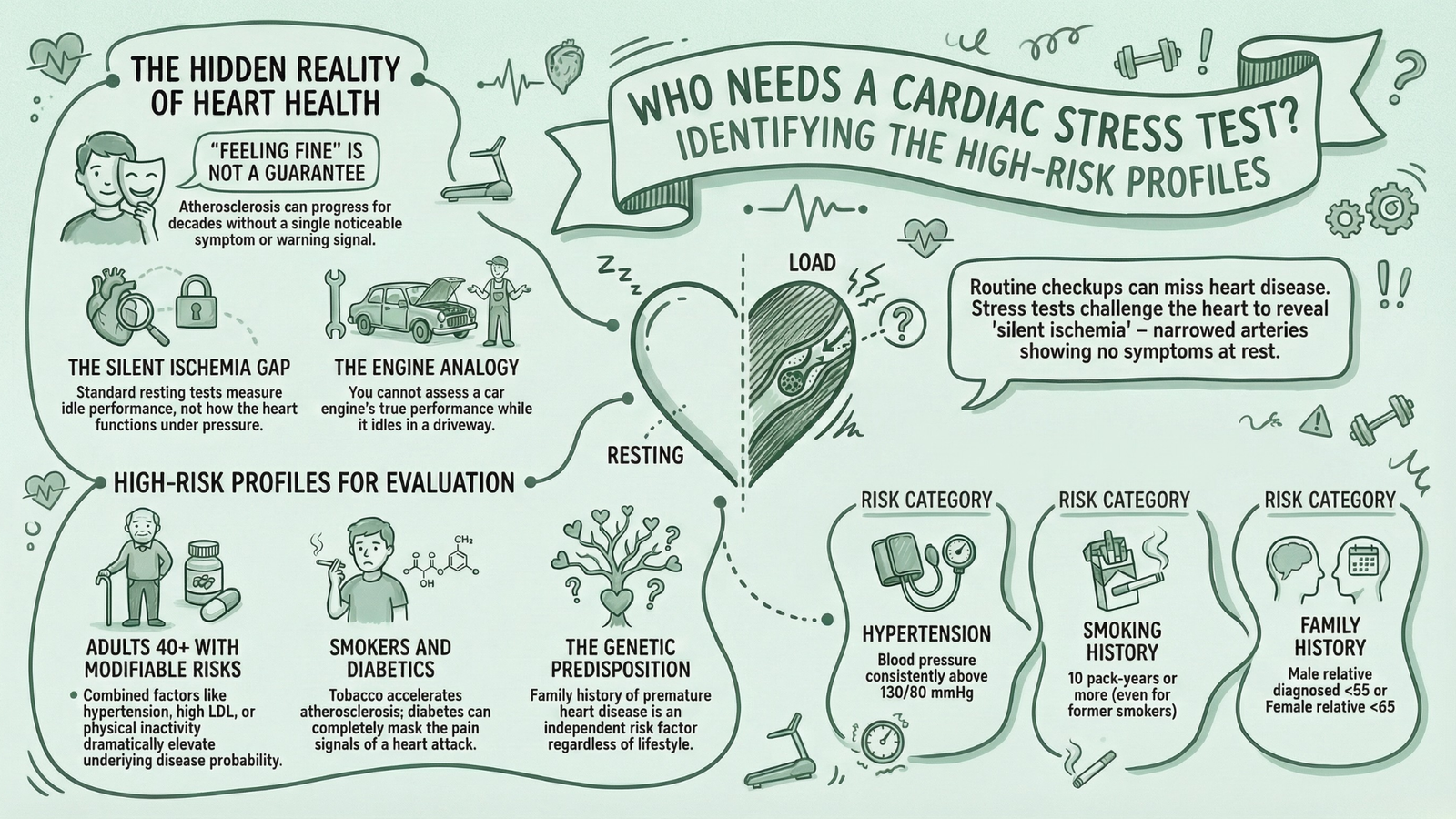
Individuals Experiencing Symptoms
Some people reading this section are not in a preventive context at all. They are experiencing symptoms right now – symptoms that may or may not be cardiac in origin, but that deserve thorough investigation regardless.
Symptoms that should prompt an urgent stress test discussion include:
- Chest pain, pressure, tightness, or discomfort – particularly if it occurs or worsens during physical activity or exertion
- Unexplained shortness of breath during activities that previously caused no difficulty
- Palpitations – an awareness of the heartbeat, irregular beats, or episodes of racing heart, particularly during exercise
- Unexplained fatigue or weakness that seems disproportionate to activity level
- Dizziness or lightheadedness during or after physical exertion
- Near-syncope or syncope – near-fainting or actual loss of consciousness during activity
Any of these symptoms, occurring in the context of physical exertion, represents a potentially cardiac presentation until proven otherwise. This is not an invitation to panic – many of these symptoms have entirely benign explanations. But it is a clear signal that cardiac evaluation, including stress testing, should happen promptly rather than being deferred.
Situations That Typically Trigger a Doctor’s Referral
Beyond the proactive, patient-initiated conversation, there are specific clinical situations in which most cardiologists will order a stress test as a standard component of care. Understanding these situations helps you recognise when to expect a referral – and when to ask why one has not been made.
Pre-Surgical Cardiac Clearance
Major non-cardiac surgery – including orthopaedic procedures, vascular surgery, abdominal operations, and others – places significant physiological stress on the cardiovascular system. Anaesthesia, fluid shifts, pain response, and the metabolic demands of healing collectively represent a substantial cardiac challenge.
For patients with known or suspected cardiac disease, or those with significant risk factors undergoing major surgery, pre-operative cardiac stress testing provides essential information about whether the heart can safely tolerate that surgical stress. An abnormal result does not necessarily mean surgery is cancelled – it means the cardiac situation is optimised beforehand, and the surgical and anaesthetic team can plan accordingly.
Before Starting an Intense Exercise Programme
This is an often-overlooked indication that applies to a surprisingly large number of people. A previously sedentary individual in their fifties who decides to begin training for a marathon, take up competitive cycling, or join a high-intensity interval training class is about to impose a dramatically increased physiological load on a cardiovascular system that has been relatively unchallenged for years.
For individuals over 40 with one or more risk factors, a stress test before beginning high-intensity exercise is a clinically reasonable – and potentially life-saving – precaution. The goal is not to discourage exercise. Exercise is profoundly beneficial for cardiovascular health. The goal is to ensure that a dangerous coronary lesion is not lurking silently, waiting to be exposed by a sudden dramatic increase in cardiac demand.
After a Cardiac Event
Following a myocardial infarction, coronary artery stenting, or bypass surgery, stress testing becomes a standard tool in the monitoring and rehabilitation arsenal. Its purposes in this context are multiple:
- Assessing residual ischemia – are there other coronary territories still at risk beyond what was treated?
- Evaluating functional capacity – what level of physical activity is safe for this patient at this point in their recovery?
- Establishing exercise prescription for cardiac rehabilitation programmes
- Confirming procedural success – is the stent patent? Are the bypass grafts functioning?
- Monitoring disease progression over subsequent years
Monitoring Known Heart Disease Progression
For patients with established coronary artery disease, stress testing at regular intervals – typically every one to three years depending on clinical stability – provides an objective measure of whether the disease is stable, progressing, or responding to treatment. A patient who was managing well two years ago may have experienced silent progression that changes their treatment plan entirely.
Who Should NOT Have a Standard Stress Test
Clinical medicine is never a blanket prescription, and stress testing is no exception. There are specific situations in which a standard exercise stress test is contraindicated – meaning the risks of performing the test outweigh its diagnostic benefits in that particular moment.
Absolute contraindications to standard exercise stress testing:
- Acute myocardial infarction within the previous 48 hours – the heart muscle is in an actively vulnerable state
- Unstable angina that has not been stabilised medically – unpredictable, ongoing ischemia makes exercise-induced stress dangerous
- Uncontrolled cardiac arrhythmias causing haemodynamic instability – the risk of precipitating a life-threatening rhythm disturbance is unacceptably high
- Severe symptomatic aortic stenosis – the outflow obstruction leaves no haemodynamic reserve for the demands of exercise
- Acute pulmonary embolism or pulmonary infarction – significant cardiovascular compromise already present
- Acute myocarditis or pericarditis – active inflammation of the heart muscle or surrounding sac
- Acute aortic dissection – an immediately life-threatening emergency incompatible with stress testing
Relative contraindications – situations requiring careful individual risk-benefit assessment before proceeding:
- Significant electrolyte abnormalities
- Severe hypertension (systolic above 200 mmHg or diastolic above 110 mmHg at rest)
- Hypertrophic cardiomyopathy – requires specialist supervision
- High-degree heart block without a pacemaker
- Significant cognitive or physical limitations affecting safe treadmill use
The important reassurance here: the existence of contraindications to the standard exercise stress test does not mean cardiac evaluation is impossible. For virtually every patient in whom exercise testing is contraindicated, a pharmacological stress test – using medication to achieve the necessary cardiovascular stress without physical exertion – represents a safe and effective alternative. The diagnostic question can almost always still be answered; only the method changes.
How to Talk to Your Doctor About Getting One
This is where many people stumble – not because they lack the inclination to advocate for themselves, but because medical appointments are short, doctors are busy, and the conversational dynamic of a clinical encounter can make it genuinely difficult to raise concerns proactively rather than reactively.
Here is a practical framework for having that conversation effectively.
Questions to Ask at Your Next Appointment
These specific questions tend to be productive in opening a meaningful cardiac evaluation discussion:
- “Given my age and risk factors, would a cardiac stress test be appropriate for me?”
- “I have been experiencing [specific symptom] during physical activity – could a stress test help determine whether this is cardiac in origin?”
- “My father had a heart attack at 54 – at what point should I be considering more proactive cardiac screening?”
- “I am planning to significantly increase my exercise intensity – do you think a stress test makes sense before I do that?”
- “When was my cardiac risk last formally assessed, and has anything in my recent results changed that picture?”
Open, specific questions are far more effective than vague expressions of concern. Arriving with concrete information – your age, your risk factors, your symptoms, your family history – and asking direct questions about whether a stress test is indicated puts you in an active role in your own cardiac care.
How to Advocate for Yourself If Your Concerns Are Dismissed
Medicine is not infallible, and dismissal of cardiac concerns – particularly in women, younger adults, and individuals from certain ethnic backgrounds – is a documented phenomenon in clinical research. If you raise a genuine concern and feel it is not being taken seriously, you have several legitimate options:
- Request a formal risk assessment using a validated tool such as the Framingham Risk Score or the ACC/AHA Pooled Cohort Equations – these tools calculate 10-year cardiovascular risk using your specific demographic and clinical data, and a high score provides objective grounds for further investigation
- Ask for the reasoning to be documented – a doctor who declines to investigate a symptom or risk factor should be willing to explain why, and that explanation should be clearly recorded in your notes
- Request a cardiology referral directly – you are within your rights to ask for a specialist opinion, particularly if your symptoms are ongoing or your risk factor burden is significant
- Seek a second opinion – this is not a confrontational act. It is a standard, accepted part of navigating complex medical decisions, and any competent physician will respect your right to do so
The goal is not adversarial. Most doctors who initially decline to order a stress test are making a reasonable clinical judgment based on incomplete information. Providing more complete information – about your symptoms, your family history, your concerns – frequently changes that assessment.
What to Expect From the Referral Process
Once a stress test is agreed upon, the practical pathway is relatively straightforward:
- Your primary care physician generates a referral to a cardiologist or directly to a cardiac diagnostic facility
- A pre-test consultation may be scheduled to review your history and determine the most appropriate type of stress test
- You receive preparation instructions covering diet, medications, and clothing
- The test is performed, typically as an outpatient procedure requiring no hospitalisation
- Results are reviewed by the cardiologist and communicated to you – usually within 1 to 5 business days, though urgent findings are acted upon immediately
- A follow-up appointment is scheduled to discuss results and any recommended next steps
The entire process, from referral to results, typically takes between one and three weeks in most healthcare systems, though urgent referrals for symptomatic patients can move considerably faster.
Frequently Asked Questions – Section 4
You now have a clear picture of who should be considering a stress test, the specific situations that warrant one, the clinical boundaries around when it should not be performed as a standard exercise test, and exactly how to initiate the process if you believe one is appropriate for your situation.
But there is one more critical piece of the puzzle – arguably the part that most people find most confusing, most anxiety-provoking, and most consequential:
What do your stress test results actually mean?
A piece of paper that says “abnormal ST changes noted at stage 3 of Bruce Protocol” means very little to the average patient without context and interpretation. In the final section of this guide, we break down exactly what normal results tell you, what abnormal findings actually mean – and what not to panic about – how to navigate the grey zone of inconclusive results, and most importantly, a clear five-step action plan for what to do after your test is complete.
What Your Stress Test Results Really Mean – And What to Do Next
You have done the hard part.
You advocated for yourself, scheduled the appointment, showed up, walked the treadmill, and made it through the electrodes and the blood pressure cuff and the gradually increasing incline. The test is done. Now comes the part that, for many people, produces more anxiety than the test itself.
The results.
A printed report filled with medical terminology, numerical values, and clinical observations that mean everything – and, without proper context, almost nothing. The difference between a result that genuinely requires urgent follow-up and one that is entirely reassuring can be subtle, and the emotional weight of waiting to understand which category you fall into is real.
This section is designed to remove that uncertainty entirely. Here is exactly what your stress test results mean, how to interpret them with clarity, and – most importantly – what you should actually do with that information.
Normal Results – What “Passing” Actually Means
Receiving a normal stress test result is genuinely good news. But it is worth understanding precisely what “normal” means in this context, because it carries both meaningful reassurance and important nuance.
A normal stress test result is defined by a cluster of findings that together indicate the heart is responding appropriately to physical demand without evidence of ischemia, dangerous arrhythmia, or significant structural dysfunction.
The Components of a Normal Result
Heart rate response within expected range:
During a standard exercise stress test, the target is to achieve at least 85% of the age-predicted maximum heart rate – calculated as 220 minus your age. A heart that accelerates appropriately through the exercise stages and reaches this target zone has demonstrated normal chronotropic competence – the ability to increase its rate in proportion to physiological demand.
Failure to reach 85% of predicted maximum – known as chronotropic incompetence – is itself a potentially significant finding, even in the absence of other abnormalities, and is associated with elevated cardiovascular risk.
No significant ECG changes during exertion:
Throughout the exercise and recovery phases, the ECG trace should remain largely stable. Minor variations are normal and expected as heart rate increases. What constitutes a significant change – the kind that flags a problem – is discussed in the abnormal results section below. A normal result means none of those changes appeared.
Appropriate blood pressure response:
Blood pressure should rise in a controlled, progressive manner during exercise – typically reaching a systolic pressure of between 160 and 200 mmHg at peak exertion in a healthy adult. It should then return steadily toward baseline during the recovery phase.
An exaggerated hypertensive response – systolic pressure exceeding 210 mmHg in men or 190 mmHg in women during exercise – may indicate latent hypertension or elevated future cardiovascular risk even in an otherwise normal test. A failure of blood pressure to rise with increasing workload, or an actual drop in pressure during exercise, is a more immediately concerning finding.
Good exercise capacity – MET score:
Achieving a strong MET score – ideally above 8–10 METs for middle-aged adults – is one of the most reassuringly positive outcomes a stress test can generate. As discussed in the previous section, exercise capacity is one of the strongest independent predictors of long-term survival available in clinical medicine. A high MET score does not just mean you passed the test – it means your cardiovascular system is functioning with genuine reserve capacity.
No symptoms during exercise:
Completing the full exercise protocol without chest pain, significant breathlessness disproportionate to workload, dizziness, or near-syncope is an important qualitative component of a normal result.
The Important Caveat – Normal Does Not Mean Zero Risk
This point deserves direct, unambiguous statement: a normal stress test result does not guarantee the absence of coronary artery disease.
The standard exercise ECG stress test has a sensitivity of approximately 68% for detecting significant coronary artery disease – meaning that roughly 32% of people with real, significant coronary obstruction will have a test that appears normal. This is not a failure of the test so much as a reflection of its mechanism: ECG changes only appear when a sufficient proportion of the heart muscle is ischemic, meaning small-vessel disease, single-vessel moderate stenosis, or early-stage atherosclerosis may not produce detectable changes.
A normal result is a strong and clinically meaningful indicator that significant, flow-limiting coronary disease is unlikely. It is not, and should not be interpreted as, a declaration of perfect cardiac health. Ongoing attention to cardiovascular risk factors – cholesterol, blood pressure, weight, activity level, smoking – remains important regardless of a normal stress test result.
Abnormal Results – Don’t Panic, But Don’t Ignore
An abnormal stress test result is not a diagnosis. It is a signal – a prompt for further investigation – and the appropriate response is calm, systematic follow-up rather than either dismissal or catastrophising.
That said, certain abnormal findings do carry genuine urgency, and it is important to understand the difference between findings that require prompt action and those that simply warrant additional clarification.
ST-Segment Depression or Elevation
ST-segment changes are the most commonly discussed ECG abnormality in the context of stress testing, and for good reason – they are the primary electrical signature of myocardial ischemia.
- Horizontal or downsloping ST depression of 1 millimetre or more, lasting at least 60–80 milliseconds beyond a specific reference point on the ECG trace, is the classic marker of exercise-induced ischemia. The depth of depression, the number of leads affected, the exercise stage at which it appears, and whether it persists into recovery all contribute to the clinical significance of the finding
- ST elevation during exercise – particularly in leads without a prior Q-wave – is a more immediately serious finding, potentially indicating severe transmural ischemia or coronary artery spasm, and typically warrants very prompt further investigation
- The distribution of ST changes across different ECG leads provides information about which coronary artery territory may be involved, guiding subsequent imaging
What happens next: Significant ST changes typically prompt referral for coronary angiography – a catheter-based procedure that directly visualises the coronary arteries and can identify the precise location and severity of any obstruction – or non-invasive coronary imaging such as CT coronary angiography (CTCA).
Chest Pain or Shortness of Breath During the Test
The development of anginal chest pain during the exercise phase – particularly if accompanied by ECG changes – significantly increases the diagnostic certainty of a positive result. The combination of symptoms and electrical changes is more specific for significant coronary disease than either finding alone.
Shortness of breath that is markedly disproportionate to the exercise workload – appearing at a very low MET level in a patient who is not severely deconditioned – may indicate significant cardiac dysfunction and warrants careful evaluation.
Abnormal Blood Pressure Response
Two blood pressure patterns are particularly significant:
- Exercise-induced hypotension – a drop in systolic blood pressure of 10 mmHg or more from baseline during exercise, or failure to rise with increasing workload – is one of the more serious stress test findings, suggesting significant left ventricular dysfunction or severe multivessel coronary disease. It can be a marker of haemodynamic compromise and may prompt urgent further evaluation
- Severely exaggerated hypertensive response – exceeding 250/115 mmHg – may prompt early termination of the test and reassessment of antihypertensive management
Serious Arrhythmias Triggered by Exertion
The development of sustained ventricular tachycardia during exercise is a potentially dangerous finding that typically prompts immediate test termination and urgent cardiac evaluation. Complex ventricular ectopy – frequent premature ventricular contractions, couplets, or runs of non-sustained VT – that appears during exercise or worsens in recovery is also a clinically significant finding requiring further investigation.
The development of high-degree heart block or new bundle branch block during exercise are additional ECG abnormalities that warrant prompt follow-up.
What Happens After an Abnormal Result
The pathway following an abnormal stress test depends on the specific findings and their severity:
- Mildly abnormal or borderline findings → Advanced stress imaging (nuclear stress test or stress echocardiogram) for clarification
- Moderately abnormal findings → CT coronary angiography for non-invasive anatomical assessment of the coronary arteries
- Significantly abnormal findings (severe ST changes, exercise-induced hypotension, sustained arrhythmia) → Invasive coronary angiography often recommended promptly
- Findings suggesting heart failure → Cardiac MRI, echocardiography, and heart failure specialist referral
The speed of follow-up is calibrated to the severity of the findings. A mild ECG abnormality in a low-risk patient may be evaluated over weeks. A strongly positive test in a patient with multiple risk factors may prompt evaluation within days.
The Grey Zone – Inconclusive Results
Not every stress test produces a neatly categorised result. A meaningful proportion of tests – estimates vary, but figures of 10–30% are commonly cited in the literature – fall into a diagnostically ambiguous territory: neither clearly normal nor definitively abnormal.
Why Inconclusive Results Happen
Several factors contribute to equivocal stress test results:
- Submaximal effort – if the patient cannot or does not reach 85% of predicted maximum heart rate, the test has not adequately challenged the cardiovascular system. The absence of abnormalities at low-to-moderate effort cannot be interpreted as confidently as their absence at peak effort
- Resting ECG abnormalities – certain pre-existing ECG patterns, including left bundle branch block (LBBB), left ventricular hypertrophy with repolarisation changes, Wolff-Parkinson-White syndrome, and the effects of digoxin therapy, make ST-segment interpretation during exercise unreliable or impossible
- Borderline ST changes – small ST changes that are present but fall just short of the conventional diagnostic threshold create genuine interpretive uncertainty
- Isolated symptoms without ECG changes – a patient who develops typical chest tightness during exercise without any accompanying ECG abnormality presents a diagnostic challenge that requires clinical judgment
False Positives – More Common in Women
False positive stress tests – results that appear abnormal but are not accompanied by significant coronary disease on subsequent angiography – are a well-documented phenomenon, and they are substantially more common in women than in men.
The reasons for this sex difference are multifactorial: women more commonly have microvascular coronary disease (disease of the small vessels rather than the major epicardial arteries), which produces symptoms and ECG changes but may not show obvious obstruction on angiography. Women also have different hormonal influences on ECG repolarisation, and referral bias in historical research has led to less precise calibration of stress test criteria for female populations.
What this means practically: A positive stress test in a woman – particularly a younger woman without significant risk factors – should be interpreted with appropriate caution and ideally confirmed with imaging-based testing before proceeding to invasive evaluation.
The Path Forward From an Inconclusive Result
An inconclusive result is not a dead end. It is a direction – toward a more specific test. The standard pathway involves:
- Upgrading to imaging-based stress testing – nuclear stress testing or stress echocardiography provides significantly higher diagnostic accuracy than standard ECG testing alone, and typically resolves the ambiguity that an inconclusive exercise ECG creates
- CT coronary angiography – in selected patients, non-invasive anatomical imaging of the coronary arteries provides a definitive answer about whether significant obstruction is present, independent of functional testing
- Holter monitoring – if the inconclusive result relates primarily to arrhythmia assessment, extended ambulatory ECG monitoring over 24–72 hours may capture rhythm abnormalities that the stress test period missed
Your 5-Step Action Plan After a Stress Test
Regardless of whether your result is normal, abnormal, or somewhere in between, there are concrete steps you should take to maximise the value of the information your stress test has generated. Here is a clear, practical framework.
Step 1: Get a Full Written Copy of Your Results and Ask for an Explanation
This sounds obvious, but a surprising number of patients receive their stress test outcome as a brief verbal summary – “everything looks fine” or “there are a few things we want to look into” – without ever receiving or reviewing the actual report.
Request the full written report. Read it. If there are terms you do not understand, ask for them to be explained in plain language. You are entitled to a complete understanding of your own diagnostic results, and a good physician will make time to provide that.
Specifically ask:
- What was my peak MET score?
- Did my heart rate reach the target zone?
- Were there any ECG changes, and if so, at what exercise stage?
- How did my blood pressure respond?
- Is any follow-up testing recommended?
Step 2: Follow Up With a Cardiologist If Any Abnormality Is Found
If your results are anything other than unequivocally normal, a follow-up appointment with a cardiologist – rather than just your primary care physician – is strongly advisable. Cardiologists have the specialist training to contextualise stress test findings within your complete clinical picture, to determine whether further investigation is warranted and what form it should take, and to initiate appropriate treatment if a significant condition has been identified.
Do not allow a mildly abnormal result to simply be filed away with a vague plan to “monitor it.” Ask specifically: What is the recommended next step, and on what timeline?
Step 3: Review and Adjust Lifestyle Factors
A stress test result – whatever it shows – is an opportunity for honest reassessment of the modifiable factors that drive cardiovascular risk. Even a normal result should prompt reflection on whether those factors are genuinely well-managed.
Key lifestyle domains to review:
- Dietary quality – Mediterranean-style eating patterns, rich in vegetables, legumes, whole grains, olive oil, and fish, have the strongest evidence base for cardiovascular risk reduction
- Physical activity – the target of 150 minutes of moderate-intensity or 75 minutes of vigorous-intensity aerobic activity per week, as recommended by major cardiac guidelines, remains the single most impactful lifestyle intervention for cardiovascular health
- Smoking cessation – if you are still smoking, no stress test result – normal or otherwise – changes the fundamental imperative to stop
- Weight management – even modest weight reduction (5–10% of body weight) produces measurable improvements in blood pressure, lipid profile, and insulin sensitivity
- Sleep quality – obstructive sleep apnoea is an underrecognised independent cardiovascular risk factor. If you snore heavily, experience daytime fatigue, or have been told you stop breathing during sleep, a sleep study is warranted regardless of your stress test result
- Stress management – chronic psychological stress drives inflammatory pathways that contribute to atherosclerosis. This is not a soft lifestyle recommendation – it is a physiological reality with clinical implications
Step 4: Revisit Medications With Your Doctor Based on Findings
If your stress test reveals that existing cardiac medications are not achieving their intended effect, that conversation needs to happen promptly.
- If you are on beta-blockers for rate control and your heart rate response during the test was poorly controlled, your dose may need adjustment
- If anti-anginal medication was expected to prevent exercise-induced ischemia and the test shows it is not doing so adequately, alternative or additional agents should be discussed
- If the test has revealed a new finding – an arrhythmia, previously undetected ischemia, valve dysfunction – new medications may now be indicated as part of your management plan
- If your test was normal but your lipid profile, blood pressure, or glycaemic control remain suboptimal, this is an appropriate moment to revisit whether your current medication regimen is sufficient
Step 5: Schedule Your Next Stress Test
A stress test is not a one-time event. It is a snapshot – a detailed and diagnostically powerful snapshot, but a snapshot nonetheless. Cardiovascular disease is dynamic; it evolves over time in response to ageing, lifestyle changes, treatment interventions, and the natural progression of underlying conditions.
General guidance on repeat testing frequency:
- Normal result, low-risk patient, no symptoms: Repeat testing in 3–5 years, or sooner if symptoms develop or risk factors change significantly
- Normal result, moderate-to-high risk patient: Discuss with your cardiologist – annual or biennial testing may be appropriate
- Abnormal result with subsequent intervention (stent, bypass): Typically retested at 1 year post-procedure, then at regular intervals thereafter
- Known coronary artery disease under medical management: Annual stress testing is common practice in many centres, though frequency should be individualised based on stability and symptom status
- Cardiac rehabilitation patients: Stress testing at programme entry and completion, with follow-up guided by clinical progress
Mark the date in your calendar. Set the reminder. And when the time comes, do not let it slip past.
Frequently Asked Questions – Section 5
Conclusion – 30 Minutes That Could Add Years to Your Life
There is a particular kind of courage involved in seeking information about your own health – especially when part of you suspects, or fears, that the answer might not be what you hoped for. The instinct to look away, to stay comfortable in the assumption that feeling fine means being fine, is entirely human.
But the heart does not care about assumptions. It operates on physiology, not optimism.
What we have covered across this complete guide represents everything you need to understand about one of cardiology’s most powerful and accessible diagnostic tools. Let us bring it together one final time.
The Invitation
A stress test is not a threat. It is not an admission that something is wrong. It is a tool – a remarkably capable, remarkably accessible tool – for generating the kind of objective, evidence-based knowledge about your cardiovascular health that no amount of optimism or assumption can replicate.
Thirty minutes on a treadmill, under careful medical supervision, monitoring your heart as it does the one thing that reveals its true condition – work.
That is all it takes.
If you are in a high-risk group, if you have symptoms that concern you, if your family history gives you reason to look more carefully, or if you simply want the peace of mind that comes from genuinely knowing – rather than merely hoping – that your heart is functioning well: talk to your doctor today.
Your heart has been working for you every single minute of your life, without pause, without complaint, without asking for anything in return.
Thirty minutes of attention seems like a reasonable exchange.

{kind=link}