What Is Ketamine Therapy? The Fast-Acting Depression Treatment Psychiatrists Can’t Ignore Anymore
Picture this. You’ve spent three years – maybe five, maybe a decade – trying to find something that works. You’ve swallowed pill after pill, adjusted doses, switched medications, sat through side effects that made everything feel worse before it got marginally better. You’ve been patient. You’ve followed the protocol. And still, every morning feels like wading through concrete.
Start ReadingWhen Antidepressants Stop Working, What Comes Next?
Picture this. You’ve spent three years – maybe five, maybe a decade – trying to find something that works. You’ve swallowed pill after pill, adjusted doses, switched medications, sat through side effects that made everything feel worse before it got marginally better. You’ve been patient. You’ve followed the protocol. And still, every morning feels like wading through concrete.
You are not alone. And more importantly, you are not out of options.
For millions of people living with treatment-resistant depression, the mental health system has felt like a revolving door – exhausting, demoralizing, and cruelly slow. But over the past decade, a treatment that once seemed too unconventional to take seriously has begun reshaping what psychiatrists believe is possible. It works differently from anything that came before it. It works fast. And the medical community, once skeptical, is paying very close attention.
That treatment is ketamine therapy.
This article is the first in a comprehensive guide designed to answer one of the most searched questions in mental health today: what is ketamine therapy, how does it work, who is it for, and – critically – should you or someone you love be considering it?
Whether you are a patient who has exhausted conventional options, a caregiver researching on someone’s behalf, a mental health professional tracking emerging treatments, or simply someone curious about a therapy that keeps appearing in the headlines, this guide was written for you.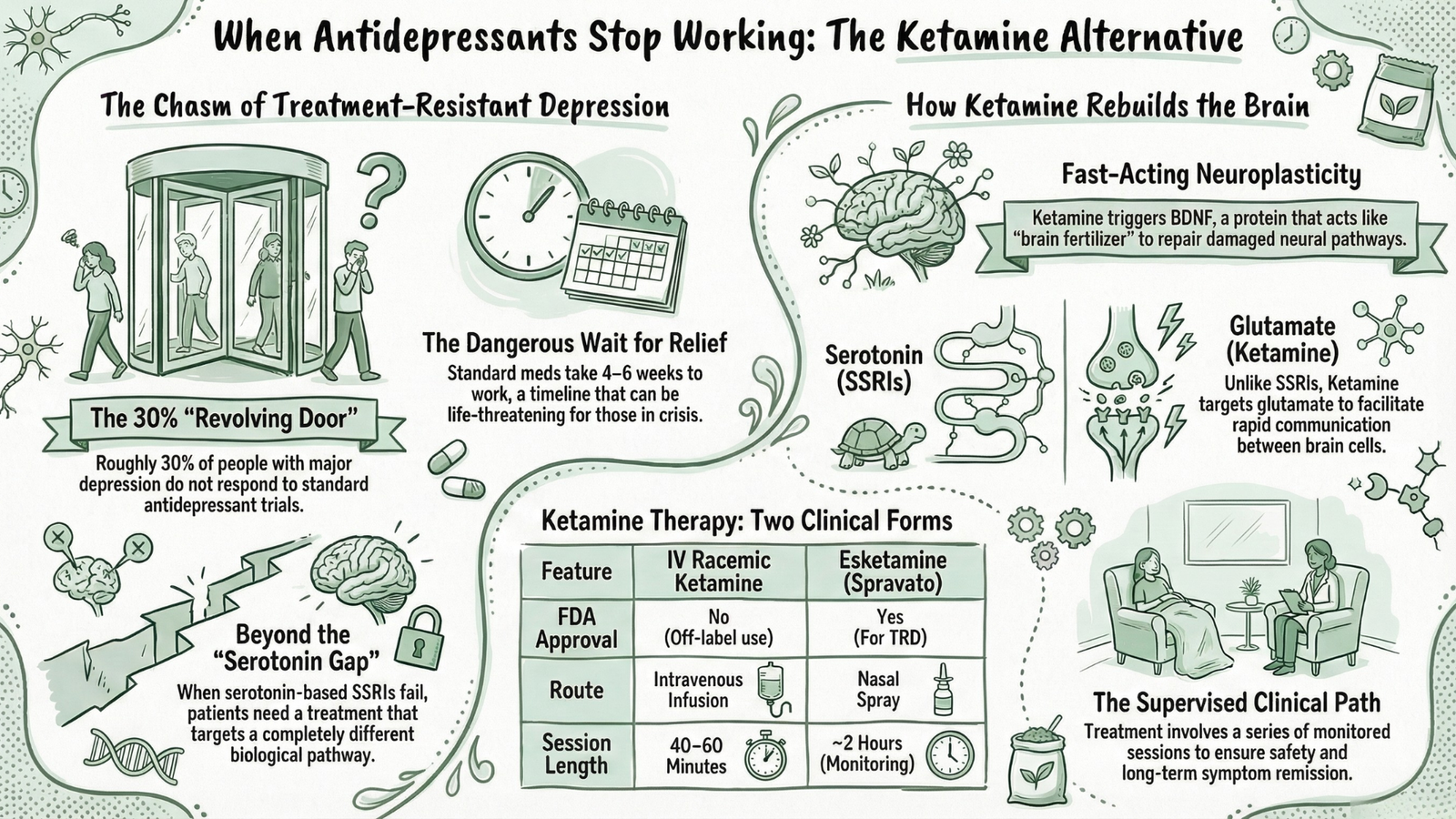
The Scale of the Problem: A Mental Health Crisis That Conventional Treatment Is Failing
Let’s start with numbers, because the numbers demand attention.
According to the World Health Organization, depression affects more than 280 million people globally, making it one of the leading causes of disability on the planet. In the United States alone, roughly 21 million adults experience at least one major depressive episode each year. These are not just statistics – they represent real people, real suffering, and real lives derailed by an illness that remains widely misunderstood and chronically undertreated.
Here is what makes this crisis particularly urgent: conventional antidepressants fail a staggering proportion of the people who need them most.
The landmark STAR*D study – one of the largest real-world trials of antidepressant treatment ever conducted – found that after trying one antidepressant, only about 37% of patients achieved remission. After a second medication trial, cumulative remission rates crept upward but plateaus quickly. By the time a patient has tried two or more antidepressants without meaningful relief, they are formally classified as having treatment-resistant depression – a condition that affects an estimated 30% of all people diagnosed with major depressive disorder.
Thirty percent. That is not a small subgroup. That is tens of millions of people worldwide for whom the standard first-, second-, and third-line treatments simply do not deliver.
And this says nothing of the patients managing:
- Post-Traumatic Stress Disorder (PTSD) rooted in complex childhood trauma or acute life events
- Bipolar depression, where mood stabilizers blunt the lows but never fully lift them
- Chronic anxiety disorders that persist despite years of therapy and medication
- Suicidal ideation so severe and persistent that every day becomes a negotiation with survival
- Chronic pain conditions that erode quality of life and feed depressive cycles in a devastating loop
For these individuals, the gap between what the mental health system currently offers and what they actually need is not a minor inconvenience. It is a chasm. And for too long, far too many people have fallen into it.
The Emotional Reality Behind the Statistics
Statistics are useful. But they can also create distance from what this crisis actually looks and feels like for the people living inside it.
Consider what treatment-resistant depression actually means in daily life. It means canceling plans – again – because getting out of bed felt genuinely impossible. It means watching your relationships strain under the weight of an illness that is invisible to everyone except you. It means sitting in your psychiatrist’s office and hearing, “Let’s try adjusting your dose,” for the fourth time, while quietly wondering whether anything will ever actually change.
It means, for some, reaching a point of such profound hopelessness that continuing to try feels harder than stopping altogether.
This is not a dramatic exaggeration. Suicide remains one of the leading causes of death among adults aged 25 to 44 in the United States, and the link between treatment-resistant depression and suicidal ideation is well-documented and deeply serious. For patients at this end of the spectrum, the slow, trial-and-error pace of conventional psychiatric treatment is not just inefficient – it can be genuinely life-threatening.
This is precisely why the speed of ketamine’s antidepressant effect is not merely an interesting clinical footnote. For a patient in crisis, a treatment that can begin working within 24 to 72 hours rather than four to six weeks is not a luxury. It is a lifeline.
The Promise That’s Turning Heads in Psychiatry
So what exactly is generating this level of excitement – and urgency – in the psychiatric community?
The answer lies in a combination of factors that, taken together, represent something genuinely unprecedented in the history of mental health treatment.
First, the speed. Traditional antidepressants – SSRIs like fluoxetine and sertraline, SNRIs like venlafaxine – operate on a timeline measured in weeks. Most clinicians recommend waiting four to six weeks before evaluating whether a medication is working, and full therapeutic benefit can take even longer. Ketamine, by contrast, has demonstrated measurable antidepressant effects within hours in clinical settings. For a field where slow progress has long been the norm, this is nothing short of revolutionary.
Second, the mechanism. SSRIs work primarily by influencing serotonin, a neurotransmitter that plays a central role in mood regulation. But ketamine operates through an entirely different biological pathway – one involving glutamate, the brain’s most abundant excitatory neurotransmitter, and a receptor known as the NMDA receptor. This distinction matters enormously. It means that patients whose brains have not responded to serotonin-based medications have a fundamentally different mechanism available to them – one that research increasingly suggests can trigger rapid neuroplasticity, literally helping the brain rebuild the neural pathways associated with mood, motivation, and resilience.
Third, the evidence base. Ketamine is no longer a fringe treatment backed only by anecdotal reports and small pilot studies. Decades of research, including randomized controlled trials published in journals like The American Journal of Psychiatry and Biological Psychiatry, have consistently demonstrated its efficacy for treatment-resistant depression. In 2019, the U.S. Food and Drug Administration (FDA) approved esketamine – a closely related compound marketed under the brand name Spravato – specifically for treatment-resistant depression, marking the first genuinely new class of antidepressant approved in over three decades.
That approval was a turning point. It signaled that ketamine therapy had crossed from the experimental margins into the mainstream of psychiatric medicine.
Fourth, the breadth of application. While depression is the most studied indication, emerging research suggests ketamine may offer meaningful benefits for a remarkable range of conditions – PTSD, obsessive-compulsive disorder, certain anxiety disorders, addiction, and chronic pain syndromes among them. The implications of this broad therapeutic potential are still being mapped, but the early signals are consistently compelling.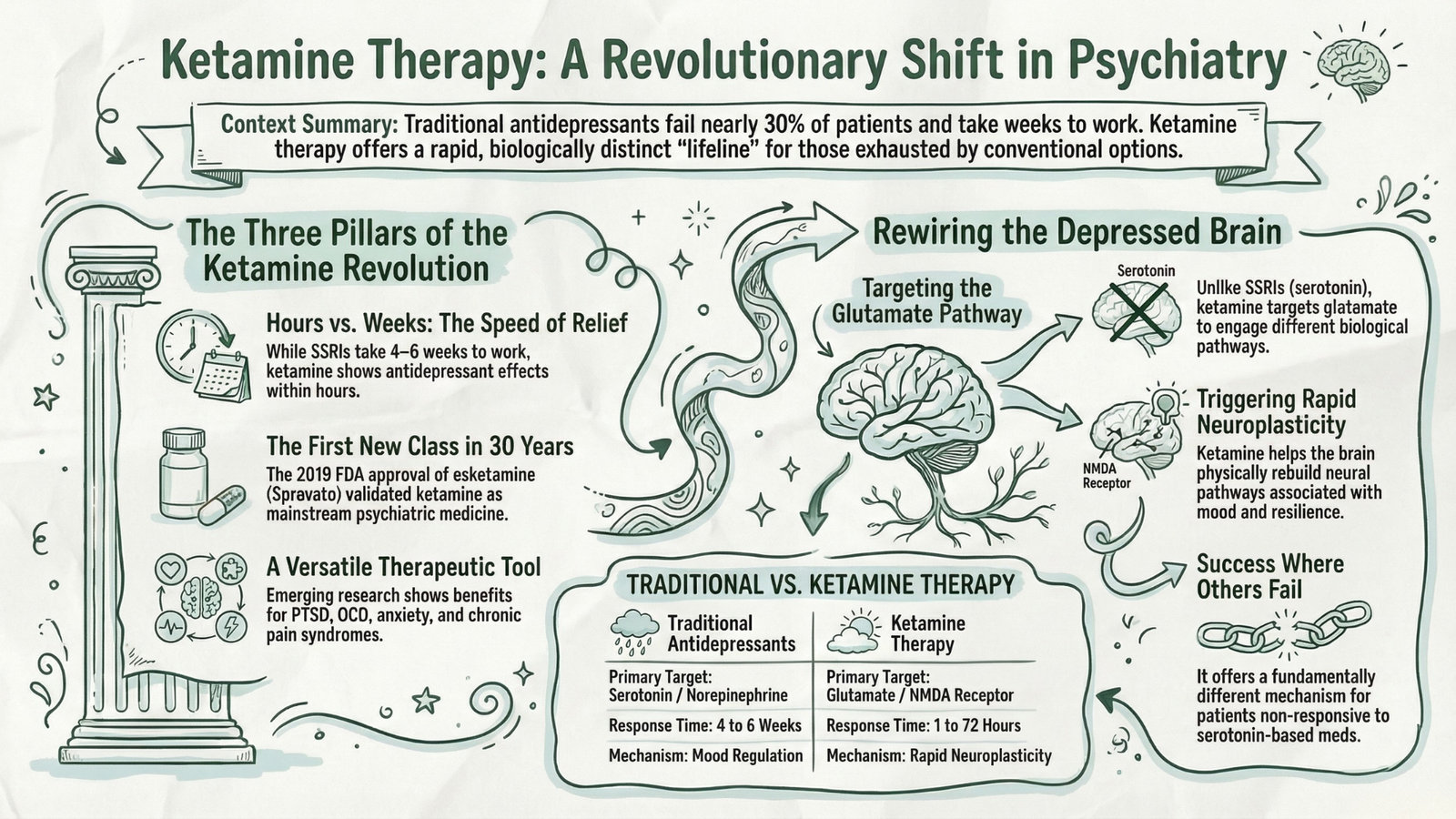
As Dr. John Krystal, Chair of Psychiatry at Yale University and one of the pioneering researchers in ketamine’s antidepressant properties, has noted, the discovery of ketamine’s rapid effects represents one of the most important advances in mood disorder research in the past fifty years. That is not marketing language. That is a measured scientific assessment from one of the most respected voices in the field.
Who This Guide Is Written For
Before going further, it is worth being direct about who will benefit most from reading this series – and what this guide is not.
This is an educational resource, not a medical recommendation. Ketamine therapy is a powerful clinical intervention that requires proper medical screening, qualified administration, and appropriate follow-up care. Nothing in this article should be interpreted as advice to seek out or self-administer any substance. If you are considering ketamine therapy, the right first step is always a conversation with a qualified psychiatrist or physician.
With that said, this guide was written for:
- Patients living with treatment-resistant depression who have tried multiple medications and are looking for an honest, thorough explanation of an alternative that their doctor may or may not have mentioned
- People managing PTSD, chronic anxiety, or suicidal ideation who want to understand whether ketamine therapy might be relevant to their situation
- Caregivers and family members of someone struggling with severe, treatment-resistant mental illness who are researching options on their behalf
- Mental health professionals who want a clear, evidence-grounded overview to share with clients or colleagues
- Curious, informed readers who have seen ketamine therapy in the news and want to understand the science and context behind the headlines
Whoever you are, and whatever brought you to this page, what you are about to read is grounded in published research, clinical evidence, and a genuine effort to present this topic with both the seriousness and the hope it deserves.
A Treatment Whose Time Has Come
The mental health landscape is changing. Slowly, unevenly, and not without controversy – but changing. The rise of ketamine therapy is part of a broader, accelerating shift in how psychiatry thinks about the brain, about consciousness, and about the tools available to treat suffering that has, for too long, been considered untreatable.
This is not a story about a miracle cure. Ketamine therapy does not work for everyone. It comes with real costs, real risks, and real limitations that deserve honest examination. Any treatment being discussed without those caveats should be regarded with healthy skepticism.
But it is a story about genuine progress. It is a story about a growing number of patients who walked into a clinic carrying years of failed treatments and walked out – days later – feeling something they had stopped believing they were capable of feeling: relief.
Understanding what ketamine therapy is, how it works, and whether it might be right for you or someone you love begins with the science – and that is exactly where we are going next.
In the next section of this guide, we go deep into the science and history of ketamine itself: what it is at a neurological level, how a surgical anesthetic developed in the 1960s became the most talked-about psychiatric intervention of the 21st century, and – in plain, jargon-free language – exactly what happens in the brain during ketamine therapy that makes rapid antidepressant effects possible. If you have ever wondered why ketamine works when so many other treatments have not, the answers are more fascinating than you might expect.
What Is Ketamine Therapy, Exactly?
Let’s be precise, because precision matters here – especially given how much confusion, stigma, and misinformation surrounds this particular compound.
Ketamine is a dissociative anesthetic – a class of drug that produces analgesia (pain relief), sedation, and, at higher doses, a profound alteration of consciousness characterized by a sense of detachment from one’s body and environment. It was synthesized in 1962, entered widespread clinical use in the 1970s, and has been on the World Health Organization’s List of Essential Medicines for decades – a designation reserved for medications considered absolutely fundamental to any functioning healthcare system.
In its anesthetic role, ketamine has an exceptional safety profile. Unlike many sedatives, it does not suppress respiratory function, which makes it invaluable in emergency medicine, battlefield surgery, and pediatric procedures where airway management is critical. This is part of why it has remained in continuous clinical use for over fifty years.
But ketamine’s role in psychiatry is something different – and something newer. In psychiatric contexts, ketamine therapy refers to the carefully controlled, clinically supervised administration of ketamine at sub-anesthetic doses specifically to treat mental health conditions, most notably treatment-resistant depression. The doses used are lower than those required for surgical anesthesia, but high enough to engage the neurological mechanisms that researchers believe drive its rapid antidepressant effects.
It is important to understand this distinction clearly, because it sits at the heart of much of the public confusion about the treatment.
FDA-Approved vs. Off-Label Use: Understanding the Distinction
This is a nuance that trips up a lot of patients – and, frankly, a lot of journalists.
When people talk about “ketamine therapy” for depression, they are often referring to one of two distinct things, and the regulatory status of each is different:
1. Racemic Ketamine (IV Infusion) – Off-Label Use
The original form of ketamine – known as racemic ketamine – contains two mirror-image molecular forms of the compound. When administered intravenously (directly into the bloodstream via IV drip) for psychiatric purposes, this constitutes an off-label use. The FDA has not formally approved IV racemic ketamine for depression. However, off-label prescribing is entirely legal and extremely common in medicine – physicians are permitted to prescribe approved drugs for conditions beyond their original approval when clinical evidence supports doing so. Thousands of licensed ketamine clinics across the United States operate on this basis, legally and legitimately.
2. Esketamine (Spravato Nasal Spray) – FDA-Approved
In March 2019, the FDA granted approval to esketamine – a refined, single-molecule derivative of ketamine, administered as a nasal spray under the brand name Spravato – specifically for treatment-resistant depression in adults. A subsequent approval for major depressive disorder with acute suicidal ideation followed in August 2020. This is the only FDA-approved ketamine-based treatment for depression, and it must be administered in a certified healthcare setting with at least two hours of post-dose monitoring required by the FDA’s risk management protocol.
Understanding this distinction matters when navigating insurance coverage, clinic legitimacy, and conversations with your own physician.
The Two Main Forms of Ketamine Therapy at a Glance
| Feature | IV Racemic Ketamine | Esketamine (Spravato) |
|---|---|---|
| FDA Approval for Depression | No (off-label) | Yes |
| Administration Route | Intravenous infusion | Nasal spray |
| Setting | Ketamine clinic / hospital | Certified healthcare facility |
| Session Duration | 40–60 minutes | ~2 hours (with monitoring) |
| Insurance Coverage | Rarely covered | Partially covered with prior auth |
| Cost | Higher out-of-pocket | More accessible with coverage |
Addressing the Stigma: Clinical Ketamine vs. Recreational Ketamine
This needs to be said plainly, because the stigma around ketamine – rooted almost entirely in its history as a recreational drug – continues to prevent some patients who might genuinely benefit from even exploring the conversation with their doctor.
Yes, ketamine is abused recreationally. Known colloquially as “Special K,” it has been used in club settings for its dissociative, euphoria-inducing effects. At high, repeated recreational doses, it can cause significant harm – including a severe condition called ketamine-induced uropathy, a form of bladder damage seen in chronic recreational users who consume quantities far exceeding anything used clinically.
None of that is relevant to what happens in a licensed clinical setting.
Therapeutic ketamine is:
- Administered at controlled, carefully calibrated doses
- Given under direct medical supervision
- Used in structured protocols with defined frequency limits
- Combined with psychological support and integration in many settings
- Monitored for adverse effects in real time
The gap between recreational abuse and supervised clinical therapy is not a narrow one – it is enormous. Morphine is also abused. Benzodiazepines are also abused. The existence of recreational misuse does not negate therapeutic value, and allowing stigma to obstruct access to a clinically validated treatment is a genuine public health failure.
A Brief History of Ketamine – From Battlefield Anesthetic to Antidepressant
The story of ketamine’s evolution from surgical tool to psychiatric breakthrough is, in many ways, a story about scientific curiosity, institutional skepticism, and the particular kind of serendipity that drives the most important discoveries in medicine.
The 1960s: Synthesis and Early Promise
Ketamine was first synthesized in 1962 by Dr. Calvin Stevens, a chemist working at Parke-Davis Pharmaceuticals, as part of a search for a safer replacement for phencyclidine (PCP) – a powerful dissociative anesthetic that caused severe and prolonged psychosis in patients. Ketamine produced a similar but far more controllable dissociative effect, with a much shorter duration of action.
It was first tested in human subjects in 1964 and quickly demonstrated a compelling safety profile. Its ability to induce anesthesia without suppressing breathing or lowering blood pressure made it almost uniquely valuable in medical contexts where standard anesthetics carried prohibitive risk.
The 1970s–1990s: Clinical Workhorse
The FDA approved ketamine for clinical use in 1970, and it rapidly became a standard tool in operating rooms, emergency departments, and military medicine. Its use during the Vietnam War – where it could be administered in field conditions without complex equipment – cemented its reputation as a robust and reliable anesthetic.
For the next three decades, ketamine was viewed almost exclusively through this lens. It was a drug that put people under for surgery and brought them back out safely. The idea that it might have relevance to psychiatry was not yet on anyone’s radar – at least, not in mainstream clinical circles.
The Late 1990s: The Psychiatric Discovery That Changed Everything
The turning point came in 1994, when researchers at Yale University – including Dr. John Krystal – began investigating ketamine’s effects on the glutamate system as part of broader research into the neurobiology of schizophrenia. What they observed was unexpected: low-dose ketamine produced transient psychotic-like symptoms in healthy volunteers, suggesting a meaningful connection between glutamate dysregulation and psychiatric illness.
This opened a door. If ketamine affected glutamate, and if glutamate was implicated in mood disorders, then perhaps ketamine had therapeutic potential far beyond the operating theater.
In 2000, Dr. Robert Berman and colleagues at Yale published what many consider the landmark study that launched the modern era of ketamine psychiatry: a small, randomized, double-blind, placebo-controlled trial demonstrating that a single intravenous infusion of ketamine produced rapid and significant antidepressant effects in patients with major depression – within hours, not weeks.
The psychiatric community’s response was a mixture of fascination and deep skepticism. The sample size was small. The effects were short-lived. And the idea of using a dissociative drug to treat depression struck many as, at best, counterintuitive.
But the data were hard to dismiss.
The 2000s–2010s: Building the Evidence Base
Over the following two decades, a steadily growing body of research corroborated and expanded on the original Yale findings. Studies at the National Institute of Mental Health (NIMH), led by Dr. Carlos Zarate, produced some of the most compelling evidence – demonstrating that ketamine could produce rapid antidepressant effects even in severely treatment-resistant patients, and that its anti-suicidal effects appeared to operate through a mechanism distinct from its general antidepressant action.
By the early 2010s, ketamine infusion clinics had begun opening across the United States – initially operating in a regulatory grey area, but gradually professionalizing as demand grew and clinical protocols matured. Patients who had exhausted every available conventional option began seeking out these clinics and, in many cases, reporting results that their psychiatrists had stopped believing were achievable.
2019: The FDA Approval That Validated a Movement
The approval of esketamine (Spravato) by the FDA in March 2019 was a watershed moment. It represented the culmination of decades of research and, perhaps more importantly, a formal institutional acknowledgment that the glutamate pathway was a legitimate and viable target for antidepressant treatment.
For the first time in over thirty years, a genuinely novel class of antidepressant had received regulatory approval. The significance of that milestone – in a field that had been cycling through variations of the same serotonin-targeting mechanisms since the 1980s – cannot be overstated.
2020–2025: Explosive Growth and Mainstreaming
The years following FDA approval have seen ketamine therapy move from the fringes of psychiatric practice into an increasingly mainstream treatment option. The number of ketamine clinics in the United States has grown dramatically. Telehealth ketamine companies – offering at-home administration of oral or sublingual ketamine – have emerged as a controversial but rapidly expanding segment of the market. Research into ketamine-assisted psychotherapy has accelerated. And the conversation around insurance coverage has intensified, with patient advocacy groups pushing insurers to recognize IV ketamine as a medically necessary treatment.
The trajectory is clear. Ketamine therapy is not a trend. It is a permanent addition to the psychiatric toolkit – and one whose role is likely to expand, not contract, in the years ahead.
How Does Ketamine Work in the Brain?
This is the question that sits at the center of everything. Understanding why ketamine works requires a brief, jargon-minimized tour of some genuinely fascinating neuroscience – and it is worth the effort, because the mechanism is not just clinically important. It is conceptually revolutionary.
The Glutamate Pathway: A Different Kind of Antidepressant
For decades, the dominant pharmacological approach to depression has been grounded in the monoamine hypothesis – the idea that depression results primarily from deficiencies or dysregulation in neurotransmitters like serotonin, dopamine, and norepinephrine. SSRIs work by blocking the reuptake of serotonin, increasing its availability in synapses. SNRIs do the same for both serotonin and norepinephrine. This approach has helped millions of people – genuinely.
But it does not help everyone. And it is slow.
Ketamine operates through an entirely different system: the glutamatergic system. Glutamate is the brain’s primary excitatory neurotransmitter – the chemical signal responsible for activating neurons and facilitating the kind of rapid, high-frequency neural communication associated with learning, memory, and synaptic plasticity.
Ketamine works primarily by blocking NMDA receptors – a specific type of glutamate receptor – in a temporary, dose-dependent fashion. This blockade triggers a cascade of downstream effects that researchers believe are responsible for its antidepressant properties.
Neuroplasticity: The Brain Rebuilding Itself
Here is where it gets particularly compelling.
One of the most significant consequences of ketamine’s action on NMDA receptors is a rapid increase in the release of BDNF – Brain-Derived Neurotrophic Factor – a protein sometimes described as “fertilizer for the brain.” BDNF plays a critical role in the survival, growth, and maintenance of neurons, and in the formation of new synaptic connections.
In people with chronic depression, research has consistently shown reduced levels of BDNF and evidence of structural changes in brain regions like the prefrontal cortex and hippocampus – areas central to mood regulation, decision-making, and emotional processing. The chronic stress response associated with depression appears to literally shrink and damage these structures over time.
Ketamine’s rapid spike in BDNF activity appears to initiate a process of neuroplasticity – the brain’s capacity to reorganize and form new neural connections. In simple terms: ketamine may help a depressed brain begin physically rebuilding the circuitry that depression has eroded. This is not a metaphor. Preclinical studies in animal models have demonstrated measurable increases in synaptic density in the prefrontal cortex following ketamine administration – structural changes occurring within hours.
The mTOR Pathway: Accelerating Neural Repair
Research has also identified the mTOR signaling pathway as a key mediator of ketamine’s rapid antidepressant effects. mTOR (mechanistic Target of Rapamycin) is a protein complex involved in regulating cell growth and protein synthesis – including the synthesis of the proteins required to build new synaptic connections.
Ketamine appears to activate mTOR signaling rapidly, accelerating the cellular machinery involved in synaptic rebuilding. This provides a plausible biological explanation for why ketamine’s effects can emerge within hours – the mTOR pathway operates on a much faster timescale than the gene transcription processes required for SSRIs to produce their effects.
Why This Mechanism Is Fundamentally Different
Ketamine is not simply “a faster antidepressant.” It is a treatment that challenges one of the oldest organizing assumptions in modern psychopharmacology.
The significance of ketamine’s mechanism cannot be overstated in the context of treatment-resistant depression. Consider what it means:
- SSRIs and SNRIs modulate serotonin and norepinephrine – systems that are either already dysregulated in treatment-resistant patients or whose dysregulation is not the primary driver of their illness
- Ketamine targets glutamate and triggers neuroplasticity – offering a biologically distinct route to symptom relief that does not depend on the same pathways that have already failed
This is not simply a “stronger” or “faster” version of the same thing. It is a fundamentally different thing. For a patient whose brain has not responded to serotonin-based interventions, ketamine is not offering more of what hasn’t worked – it is offering something their brain hasn’t encountered before.
Quick Reference: Key Neuroscience Terms
- NMDA Receptor: A glutamate receptor that ketamine temporarily blocks, initiating its antidepressant cascade
- Glutamate: The brain’s primary excitatory neurotransmitter; the system ketamine primarily targets
- BDNF: Brain-Derived Neurotrophic Factor; a protein that supports neuron growth and synaptic formation, rapidly elevated by ketamine
- Neuroplasticity: The brain’s ability to form new neural connections; believed to be central to ketamine’s antidepressant mechanism
- mTOR Pathway: A cellular signaling pathway involved in protein synthesis and synaptic rebuilding, activated by ketamine
Now that we have established what ketamine is, where it came from, and what it does at a neurological level, the natural next question is: what does all of this actually look and feel like for the patient sitting in the chair? In the next section, we walk through a ketamine therapy session from start to finish – what happens when you walk through the door, what the dissociative experience is actually like, how ketamine-assisted psychotherapy differs from standard infusion, and what to look for – and watch out for – when choosing a provider. The patient experience is where the science becomes human, and it is where many people’s most important questions begin.
What Does a Ketamine Therapy Session Actually Look Like?
For many people, the uncertainty around what ketamine therapy physically involves is one of the biggest barriers to seriously considering it. The word “ketamine” carries cultural baggage. The idea of an altered state of consciousness in a clinical setting sounds, to many ears, somewhere between alarming and bizarre. And because the experience is genuinely unlike anything most people have encountered in conventional medical care, the imagination tends to fill the gaps with worst-case scenarios.
The reality is considerably more measured – and for most patients, considerably more manageable – than the anticipation suggests.
Let’s walk through it, step by step.
Before the Session: Screening, Preparation, and What to Expect
A reputable ketamine provider will never schedule you for an infusion without first conducting a thorough medical and psychiatric evaluation. This is not a formality. It is a clinically essential process designed to establish whether you are an appropriate candidate, identify any contraindications, and set realistic expectations for the treatment.
This intake process typically includes:
- A comprehensive review of your psychiatric history – diagnoses, previous medications, treatment responses, and current symptom severity
- A medical history assessment covering cardiovascular health, kidney and bladder function, substance use history, and current medications
- A discussion of your goals and expectations – what you are hoping ketamine therapy will and will not do
- Informed consent documentation covering the nature of the experience, known risks, and post-session requirements
- In many clinics, a preparatory consultation with a therapist or integration specialist, particularly in practices offering ketamine-assisted psychotherapy
On the day of your session, you will typically be asked to fast for several hours beforehand to reduce the risk of nausea – one of the more common side effects. You will need to arrange transportation, as driving after a ketamine session is not permitted. Comfortable, loose clothing is usually recommended. Some providers suggest bringing headphones and a personal playlist of calming music, as auditory environment during the session can meaningfully shape the experience.
The Session Itself: A Step-by-Step Walkthrough
Setting and Environment
Ketamine infusion clinics vary in their aesthetic and atmosphere, but the best ones share a common philosophy: the environment matters. You are not walking into a standard hospital room. Most reputable clinics invest considerable thought into creating a space that feels calm, safe, and conducive to an introspective experience.
Expect, typically:
- A reclining chair or medical bed in a private or semi-private room
- Dimmed lighting or the option to use an eye mask
- Calming background music – many clinics have curated playlists, and some allow you to use your own
- A call button or direct staff access throughout the session
- Continuous vital sign monitoring – blood pressure and heart rate are tracked throughout, as ketamine can produce transient elevations in both
The atmosphere is deliberately designed to be neither clinical and sterile nor casually informal. The goal is a contained, supportive environment in which an altered state of consciousness can unfold safely.
IV Placement and Dosing
For intravenous ketamine infusions – the most common form of therapeutic ketamine in dedicated ketamine clinics – a nurse or physician will place an IV line, typically in your forearm. The ketamine is then administered via a controlled infusion pump at a carefully calculated dose, usually based on your body weight.
Standard antidepressant dosing for IV ketamine is typically in the range of 0.5 mg/kg administered over 40 minutes, though protocols vary between providers. This is substantially below the dose required for surgical anesthesia – enough to produce meaningful dissociative and antidepressant effects without rendering you unconscious.
A physician or trained medical professional remains present or immediately available throughout the infusion. Your vital signs are monitored continuously. The rate of infusion can be adjusted or stopped entirely if you experience significant distress.
Duration and Standard Protocol
A single IV ketamine infusion session typically lasts 40 to 60 minutes from the start of the infusion, with an additional recovery period of 30 to 60 minutes afterward before you are cleared to leave.
For treatment-resistant depression, the standard induction protocol involves six infusions administered over two to three weeks – typically three sessions per week for two weeks, or a slightly more spaced schedule depending on the provider’s approach and your response. This concentrated initial series is designed to produce and sustain the neuroplastic changes associated with antidepressant response.
After the induction series, many patients require maintenance infusions – typically administered monthly or every six to eight weeks – to sustain the benefits, though the frequency varies considerably between individuals.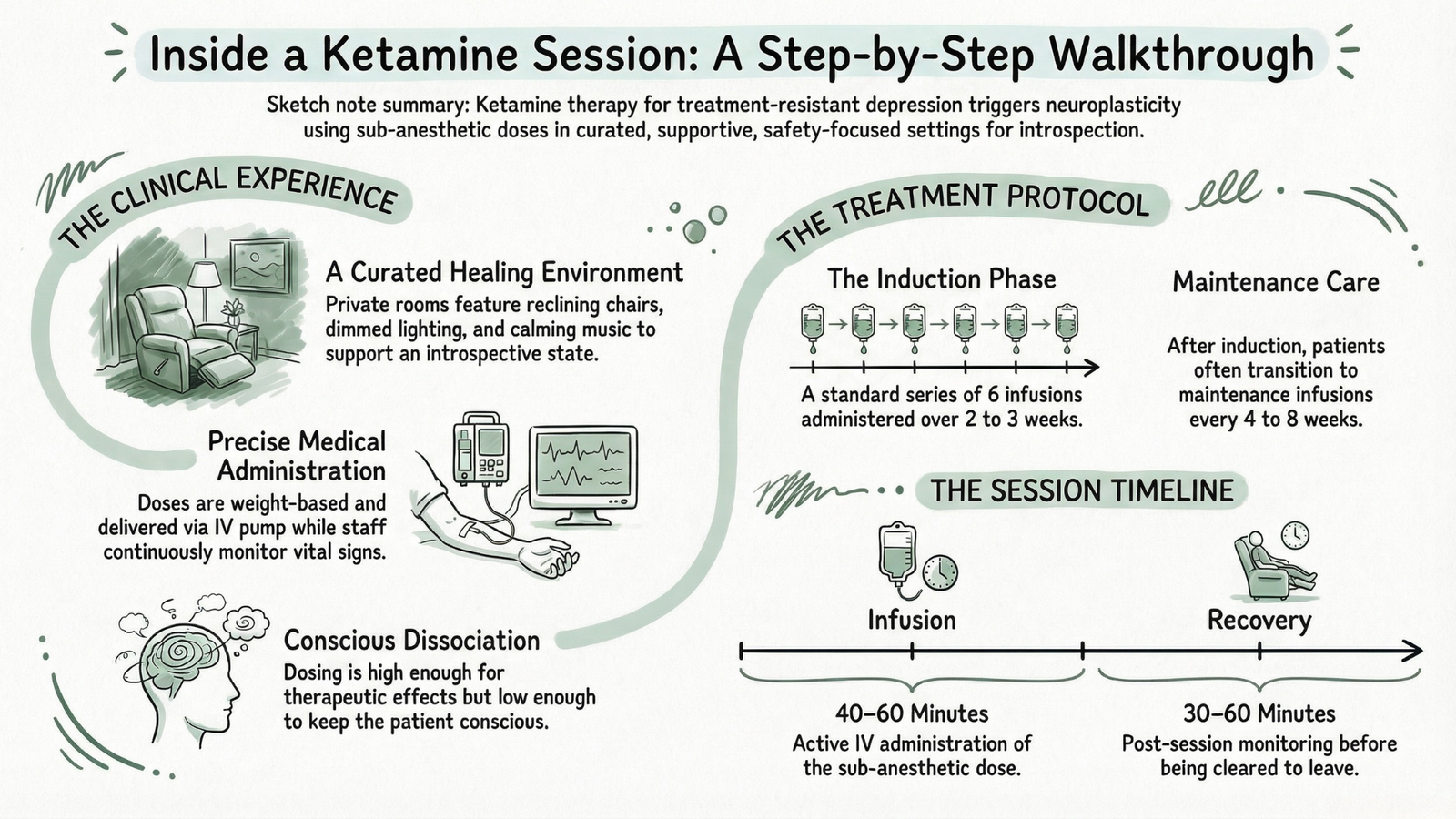
What Does Ketamine Feel Like? The Dissociative Experience Explained
This is the question most patients are simultaneously most curious about and most anxious about. And it deserves a direct, honest answer – not a sanitized one.
Ketamine at therapeutic doses produces a dissociative experience. This is not an incidental side effect. It is a pharmacological property of the drug that many researchers believe is actively therapeutic rather than merely accompanying the treatment. Understanding what dissociation actually feels like – and why it is not the same as losing control or being unconscious – is important for managing the anticipatory anxiety that many first-time patients experience.
What Patients Commonly Report
The experience varies meaningfully between individuals – and even between sessions for the same individual – but common themes emerge consistently across patient accounts:
Perceptual Changes:
- Visual distortions – objects may appear to shift, blur, or take on unusual qualities; eyes-closed visual imagery is common and can range from abstract geometric patterns to vivid, dreamlike scenes
- Altered perception of time – most patients report that time feels stretched, slowed, or loses its normal structure entirely; a 40-minute session can feel like hours or like minutes
- Altered perception of space – the room may feel larger or smaller than it is; the boundaries of your body may feel less defined or even absent
- Auditory changes – music heard during the session often takes on an unusual richness or emotional resonance; voices may sound different
Sense of Self and Consciousness:
- A profound sense of detachment from the body – sometimes described as floating, weightlessness, or observing oneself from a distance
- Dissolution of the ordinary sense of self – what researchers sometimes call “ego dissolution” – which patients describe in widely varying terms: peaceful, strange, disorienting, or deeply illuminating
- A feeling of being somehow outside normal thought patterns – detached from the rumination, self-criticism, and cognitive loops that characterize depressive thinking
Emotional Experiences:
- Many patients report feelings of profound calm, peace, or even euphoria – a sense of emotional spaciousness that can feel almost foreign to someone accustomed to chronic depression
- Others experience moments of unexpected emotional clarity – a sudden ability to see personal situations, relationships, or long-held beliefs from a new perspective
- Some patients experience brief periods of anxiety or disorientation, particularly early in their first session, before the experience settles
It is worth being honest: not every ketamine session is uniformly pleasant. Some patients encounter confusing, uncomfortable, or emotionally challenging material during the experience. This is not necessarily a sign that something has gone wrong – in therapeutic contexts, difficult experiences can be the most transformative ones – but it underscores the importance of proper clinical support and integration work.
Why the Dissociative Experience May Itself Be Therapeutic
This is an area of active and genuinely fascinating research. For many years, scientists assumed that ketamine’s antidepressant effects were purely biochemical – driven by its action on NMDA receptors and the downstream neuroplastic changes it triggers – and that the dissociative experience was simply a side effect to be managed.
Increasingly, the evidence suggests this may be wrong.
A growing body of research indicates that the subjective experience during ketamine sessions may contribute meaningfully to therapeutic outcomes – particularly in the context of depression, PTSD, and trauma-related conditions. The temporary dissolution of rigid self-referential thinking patterns, the sense of perspective gained during ego dissolution, the emotional processing that can occur in the dissociative state – these experiential dimensions may amplify and deepen the neurobiological effects of the drug itself.
This is one of the central arguments behind ketamine-assisted psychotherapy (KAP), which we will examine in detail shortly.
Integration Therapy: The Often-Overlooked Piece of the Puzzle
Whether or not a patient pursues formal ketamine-assisted psychotherapy, integration – the process of making meaning from and building on the ketamine experience – is a component that far too many clinics currently underemphasize.
Integration therapy refers to the work done between and after ketamine sessions to process whatever thoughts, emotions, imagery, or insights arose during the experience and translate them into lasting change. It is typically conducted with a trained therapist familiar with non-ordinary states of consciousness, and it can take many forms – traditional talk therapy, somatic approaches, journaling, mindfulness practices, or trauma-informed modalities.
The logic is straightforward: ketamine appears to create a window of enhanced neuroplasticity – a period of heightened openness to change in the brain’s circuitry. Without intentional effort to leverage that window, its therapeutic potential is not fully realized. With skilled integration support, the changes initiated during the ketamine experience can be deepened, reinforced, and translated into durable shifts in thought patterns, behavior, and emotional regulation.
Patients who report the most sustained benefit from ketamine therapy almost universally describe integration support – formal or informal – as a meaningful part of their experience. This is not an optional add-on. For many people, it is the difference between symptom relief that fades within weeks and transformation that holds.
Ketamine-Assisted Psychotherapy (KAP): The Next Level
Ketamine-Assisted Psychotherapy represents the most sophisticated and therapeutically ambitious application of ketamine in clinical practice. It combines the neurobiological effects of the drug with structured psychotherapeutic work conducted during or around the ketamine experience – and the evidence for its efficacy, particularly in trauma-related conditions, is compelling.
What KAP Actually Involves
In a KAP protocol, the ketamine experience is not simply monitored – it is therapeutically engaged. A trained therapist works with the patient before, during, and after the ketamine session to:
- Establish therapeutic intentions beforehand – identifying the emotional or psychological material the patient wants to explore or process
- Provide therapeutic presence during the session – offering grounding, support, and gentle guidance if the patient encounters difficult material while in the dissociative state
- Conduct integration sessions afterward – typically multiple sessions following each ketamine administration – to process the experience, extract insight, and translate shifts in perspective into concrete behavioral and relational changes
The dissociative window created by ketamine appears to lower the psychological defenses that typically make trauma processing difficult or impossible in standard talk therapy. Patients who have been unable to access or discuss traumatic material in years of conventional psychotherapy sometimes find that the ketamine state allows them to approach that material with a degree of distance and equanimity that makes engagement possible.
Who KAP Is Particularly Well-Suited For
While KAP can theoretically benefit anyone undergoing ketamine therapy, the evidence base and clinical consensus currently suggest it is particularly valuable for:
- PTSD and complex trauma – where the dissociative distance from traumatic memory can facilitate processing that traditional exposure approaches have failed to achieve
- Existential distress – including end-of-life anxiety, grief, and the kind of pervasive meaninglessness that often accompanies treatment-resistant depression
- Addiction and substance use disorders – where ketamine’s ability to disrupt rigid behavioral patterns and facilitate perspective shifts may support the motivational and psychological dimensions of recovery
- Treatment-resistant depression with significant psychological or relational components – where neurobiological intervention alone may be insufficient
KAP vs. Standard Ketamine Infusion: Key Differences
| Feature | Standard Ketamine Infusion | Ketamine-Assisted Psychotherapy |
|---|---|---|
| Primary Focus | Neurobiological symptom relief | Neurobiological + psychological transformation |
| Therapist Involvement | Monitoring only | Active therapeutic engagement |
| Session Structure | Infusion + recovery | Preparation + infusion + integration |
| Best For | TRD, acute symptom relief | Trauma, PTSD, existential distress |
| Cost | Lower | Higher (therapy fees additional) |
| Evidence Base | Strong for depression | Growing, especially for PTSD |
Who Administers Ketamine Therapy and Where?
The question of who provides ketamine therapy and where it is administered is one of the most practically important questions a prospective patient can ask – and one where the quality and rigor of the answers vary enormously across providers.
Types of Qualified Providers
Ketamine therapy should be administered only by – or under the direct supervision of – a licensed medical professional with specific training in its clinical use. This typically includes:
- Anesthesiologists – whose training in ketamine as a surgical anesthetic gives them deep pharmacological familiarity with the drug and its physiological effects
- Psychiatrists – particularly those with subspecialty interest in treatment-resistant mood disorders and, ideally, specific training in ketamine-assisted treatment
- Emergency medicine physicians – who often have extensive experience with ketamine in acute care settings
- Ketamine-certified physicians – practitioners in other specialties who have completed specific training programs in ketamine therapy administration and monitoring
For KAP specifically, the therapeutic component must be provided by a licensed therapist – psychologist, licensed clinical social worker, or licensed professional counselor – with specific training in psychedelic-assisted therapy and non-ordinary states of consciousness. The prescribing physician and therapist may or may not be the same person, depending on the model.
Clinical Settings
- Dedicated ketamine infusion clinics – the most common setting in the US, ranging from small independent practices to multi-location networks. Quality varies considerably; accreditation status and physician oversight are key markers to investigate
- Psychiatric practices – an increasing number of psychiatrists are integrating ketamine infusion into their practice, which offers the advantage of continuity with your existing mental health care team
- Hospital-based programs – typically offering the highest level of medical oversight, most commonly available for esketamine (Spravato) and for patients with complex medical profiles
- Academic medical centers – often running research protocols alongside clinical treatment, offering access to cutting-edge approaches and rigorous oversight
Telehealth Ketamine: Convenience vs. Caution
The emergence of telehealth ketamine companies – platforms that prescribe oral or sublingual ketamine for at-home administration – represents one of the most contested developments in this space.
Companies like Mindbloom, Wondermed, and others offer a model in which patients complete a remote psychiatric evaluation, receive a prescription for oral ketamine, and self-administer the medication at home while on a video call with a guide or monitor. The appeal is obvious: dramatically lower cost and barrier to access compared to in-clinic IV infusion.
The concerns are equally real:
- Oral ketamine has weaker and less predictable bioavailability than IV administration – the antidepressant evidence base is substantially thinner
- Self-administration without direct medical oversight removes the safety net that in-clinic monitoring provides
- The integration and psychotherapy components are often minimal or absent in lower-cost telehealth models
- Risk of misuse is meaningfully higher when controlled substances are dispensed for unsupervised home use
Telehealth ketamine is not inherently illegitimate. For some patients – particularly those in geographically underserved areas or with financial constraints – it may represent a meaningful and appropriate entry point. But it is not equivalent to supervised IV infusion therapy, and prospective patients deserve to understand that distinction clearly before choosing a provider.
What to Look For in a Reputable Ketamine Provider
Before committing to any ketamine clinic or provider, a thorough prospective patient should investigate:
- ✅ Direct physician oversight throughout sessions – not just a nurse with a doctor on call
- ✅ Comprehensive intake screening – a provider who schedules you without a thorough medical and psychiatric evaluation is a red flag
- ✅ Clear, written informed consent – risks, benefits, alternatives, and the nature of the experience should be explained in detail before any treatment begins
- ✅ Integration support offerings – whether the clinic offers or recommends integration therapy
- ✅ Transparent pricing and protocols – reputable providers are clear about costs, session structure, and what their treatment protocols involve
- ✅ Verifiable physician credentials – board certification, relevant training, and professional affiliations should be readily available
- ✅ Emergency protocols – the clinic should have clear procedures for managing adverse events
Red flags to watch for:
- ❌ Pressure to commit to a full treatment package before completing intake screening
- ❌ Providers unwilling to communicate with your existing psychiatrist or physician
- ❌ Minimal or no monitoring during sessions
- ❌ Vague or evasive answers to questions about physician oversight and credentials
- ❌ Promises of guaranteed outcomes or “cure” language
Understanding the patient experience of ketamine therapy – from the first consultation to the last integration session – gives you a meaningful framework for evaluating whether this treatment might be right for you or someone you care about. But the experience in the chair is only part of the picture. Equally important are the questions of who is a good candidate for ketamine therapy, what conditions it has the strongest evidence for treating, what it realistically costs, and what the genuine risks look like when examined honestly and completely. These are exactly the questions we tackle in the next section – a clear-eyed, evidence-grounded look at eligibility, costs, and the full risk profile of ketamine therapy.
Who Can Benefit From Ketamine Therapy?
One of the most common questions prospective patients ask – and one of the most important to answer honestly – is deceptively simple: is ketamine therapy actually for me?
The answer depends on a careful, individualized assessment of your diagnosis, medical history, previous treatment responses, and personal circumstances. Ketamine therapy is not a universal solution, and responsible providers will tell you so plainly. But for a specific and substantial population of patients, the evidence supporting its use is genuinely strong – and in some cases, stronger than anything else currently available.
Let’s examine who that population is, condition by condition.
Treatment-Resistant Depression (TRD): The Gold Standard Use Case
Treatment-resistant depression remains the primary and best-evidenced indication for ketamine therapy – the condition for which the scientific literature is deepest, the clinical consensus is strongest, and the FDA has formally acted through the approval of esketamine.
By clinical definition, TRD is major depressive disorder that has failed to respond adequately to at least two different antidepressant treatments of adequate dose and duration. In practice, many patients seeking ketamine therapy have tried far more than two – cycling through SSRIs, SNRIs, tricyclics, MAOIs, augmentation strategies, and combinations thereof over years or even decades without achieving sustained remission.
For this population, the ketamine evidence base is compelling. Multiple randomized controlled trials have demonstrated response rates of 50–70% in TRD patients following a standard induction series – a figure that compares favorably to virtually any other intervention available for this notoriously difficult-to-treat population. The speed of response – measurable within 24 hours in many patients – is without parallel in pharmacological psychiatry.
This is not a treatment of last resort in the sense of desperation. It is a treatment of clinical appropriateness – one that is increasingly being discussed earlier in the treatment algorithm as evidence mounts and access improves.
Major Depressive Disorder with Suicidal Ideation: A Critical Application
Perhaps the most urgent application of ketamine therapy – and one that deserves particular emphasis – is its use in major depressive disorder accompanied by acute suicidal ideation.
The conventional psychiatric response to a patient in suicidal crisis typically involves hospitalization, crisis intervention, and medication adjustments that may take weeks to produce effect. The gap between the moment of crisis and the onset of pharmacological relief is a period of profound vulnerability.
Ketamine’s rapid anti-suicidal effects appear to operate through a mechanism at least partially independent of its general antidepressant action. Multiple studies have demonstrated measurable reductions in suicidal ideation within hours of a single ketamine infusion – a timeline that no conventional antidepressant can approach. The FDA’s 2020 approval of esketamine specifically for major depressive disorder with acute suicidal ideation or behavior was a direct acknowledgment of this evidence.
This application does not mean ketamine is appropriate as a standalone crisis intervention without broader support. But for patients caught in the dangerous gap between crisis and conventional treatment response, it represents a clinically meaningful option that psychiatrists managing high-risk patients should have firmly in their toolkit.
Bipolar Depression: Emerging Evidence and Important Caveats
The use of ketamine therapy in bipolar depression – the depressive phase of bipolar disorder – is an area of genuine promise accompanied by genuine caution.
The depressive episodes of bipolar disorder are often the most debilitating and the most difficult to treat. Standard antidepressants are frequently avoided in bipolar patients due to the risk of precipitating manic or hypomanic episodes or destabilizing mood cycling. This leaves a therapeutic gap that mood stabilizers and atypical antipsychotics do not always adequately fill.
Emerging research suggests ketamine may produce rapid antidepressant effects in bipolar depression without the same risk of mood switch seen with traditional antidepressants – though the evidence is less robust than for unipolar TRD, and individual risk profiles vary considerably. Most experts recommend that ketamine in bipolar depression should only be considered under the close supervision of a psychiatrist experienced in both bipolar disorder and ketamine therapy, with careful monitoring for mood destabilization.
This is not a contraindication – but it is a context requiring significantly more clinical nuance than straightforward unipolar TRD.
PTSD and Trauma: Why Ketamine’s Memory Reconsolidation Effect Matters
Post-Traumatic Stress Disorder represents one of the most exciting emerging frontiers for ketamine therapy – and the neuroscience behind why it might work is particularly fascinating.
At its core, PTSD involves the pathological encoding and persistence of traumatic memories – memories that intrude, overwhelm, and reorganize the nervous system around a state of chronic threat response. Standard treatments including prolonged exposure therapy, EMDR, and various pharmacological approaches help many patients but leave a significant proportion with persistent, disabling symptoms.
Ketamine’s relevance to PTSD operates on multiple levels:
- Its rapid antidepressant and anxiolytic effects address the depressive and anxiety dimensions of PTSD symptomatology directly
- Its action on NMDA receptors intersects with the neurobiology of memory reconsolidation – the process by which stored memories are temporarily destabilized and then re-encoded when recalled. Research suggests ketamine may interfere with the reconsolidation of fear memories, potentially reducing their emotional charge without erasing the memories themselves
- The dissociative state it produces may allow patients – particularly in KAP contexts – to approach traumatic material with a degree of psychological distance that makes processing possible when direct engagement has previously been overwhelming
Clinical trials specifically targeting PTSD with ketamine are ongoing, and early results are encouraging. The combination of ketamine with trauma-focused psychotherapy – the KAP model discussed in the previous section – is considered by many researchers to be the most promising application of this particular combination.
Anxiety Disorders: OCD, GAD, and Social Anxiety
The evidence base for ketamine in anxiety disorders is less developed than for depression and PTSD, but it is growing – and the clinical rationale is sound.
- Obsessive-Compulsive Disorder (OCD): Several small trials have demonstrated rapid, if often transient, reductions in OCD symptom severity following ketamine infusion. The glutamatergic hypothesis of OCD – which implicates NMDA receptor dysregulation in the pathophysiology of the disorder – provides a plausible mechanistic rationale
- Generalized Anxiety Disorder (GAD): Patients with GAD frequently present alongside depression, and many report meaningful anxiety reduction as a secondary benefit of ketamine treatment undertaken primarily for depressive symptoms
- Social Anxiety Disorder: Early research is limited but suggests potential benefit, particularly given ketamine’s effects on the threat-processing circuitry implicated in social anxiety
For anxiety disorders as standalone indications – without co-occurring depression – ketamine therapy remains more experimental, and most providers would consider it only after conventional treatments have been adequately trialed.
Chronic Pain Conditions: A Different Mechanism, Real Results
Ketamine’s original role as an anesthetic and analgesic gives it a distinct advantage in the treatment of certain chronic pain conditions – one that operates through mechanisms separate from its psychiatric applications.
Conditions showing the strongest evidence include:
- Complex Regional Pain Syndrome (CRPS): One of the most painful and treatment-resistant chronic pain conditions known. Multiple studies and clinical case series support ketamine infusion – often at higher doses and longer durations than psychiatric protocols – as a meaningful intervention for patients who have failed conventional pain management
- Fibromyalgia: Evidence is more mixed, but some patients report significant and sustained pain reduction following ketamine treatment
- Neuropathic pain: Including diabetic peripheral neuropathy and post-herpetic neuralgia, where NMDA receptor involvement in central sensitization makes ketamine a pharmacologically rational choice
- Migraine and cluster headache: Emerging evidence, particularly for refractory cases
It is worth noting that chronic pain protocols typically involve different dosing strategies, session durations, and provider expertise than psychiatric protocols. A clinic specializing in depression treatment is not automatically qualified to manage complex pain conditions, and vice versa.
Addiction and Substance Use Disorders: Early But Promising Research
Perhaps the most unexpected application of ketamine therapy is in the treatment of addiction and substance use disorders – and the research, while early, is generating genuine excitement.
Studies have examined ketamine’s potential in:
- Alcohol use disorder – where ketamine appears to reduce cravings and support abstinence maintenance, possibly through its effects on memory reconsolidation of addiction-associated cues
- Cocaine and stimulant dependence – early trials suggest ketamine may disrupt the conditioned behavioral patterns associated with stimulant use
- Opioid use disorder – as an analgesic alternative that may reduce opioid requirements and potentially address the underlying pain conditions driving opioid use
The mechanisms are thought to involve both neuroplasticity – helping the brain’s reward circuitry reorganize away from addiction patterns – and the psychological dimension of the ketamine experience itself, which can produce profound shifts in perspective on one’s relationship with substances. This is an area to watch closely as larger trials report results.
Who Should NOT Use Ketamine Therapy?
Intellectual honesty requires equal clarity about contraindications. Ketamine therapy is not appropriate for everyone, and a provider who does not rigorously screen for the following conditions should be regarded with serious skepticism.
Absolute and Strong Contraindications
Active Psychosis or Schizophrenia Spectrum Disorders
This is the firmest contraindication in ketamine therapy. Because ketamine’s dissociative and perceptual effects can mimic and exacerbate psychotic symptoms, its use in patients with active psychosis or schizophrenia carries a meaningful risk of precipitating or worsening psychotic episodes. Patients with a personal or significant family history of schizophrenia or schizoaffective disorder should discuss this risk carefully with a qualified psychiatrist before any consideration of ketamine treatment.
Uncontrolled Hypertension or Significant Cardiovascular Disease
Ketamine produces reliable, dose-dependent increases in heart rate and blood pressure – a physiological effect that is manageable and monitored in healthy patients but potentially dangerous in those with uncontrolled hypertension, recent cardiac events, severe coronary artery disease, or aortic aneurysm. Cardiovascular stability must be established before treatment is considered.
Active Substance Use Disorder Involving Ketamine
While ketamine is being explored as a treatment for some substance use disorders, active ketamine abuse or dependence is a clear contraindication for therapeutic use. Providers should screen carefully for current and historical substance use – not to judge, but because the risk-benefit calculation changes fundamentally in this context.
Pregnancy and Breastfeeding
Ketamine’s effects on fetal development are not sufficiently studied to establish safety, and it is classified as a Category B drug in pregnancy with insufficient human data for confident use. Breastfeeding women should also avoid ketamine treatment due to unknown transfer through breast milk.
Certain Medications: Dangerous Interactions
Several medication classes interact meaningfully with ketamine and require careful management:
- Monoamine Oxidase Inhibitors (MAOIs): Risk of dangerous serotonergic interactions
- Benzodiazepines at high doses: May blunt ketamine’s antidepressant effects
- Stimulants and sympathomimetics: May amplify cardiovascular effects
- Lamotrigine: Some evidence suggests it may reduce ketamine’s efficacy
A complete medication review by a qualified physician before initiating ketamine therapy is not optional – it is essential.
How Much Does Ketamine Therapy Cost?
Cost is, for many patients, the most significant practical barrier to accessing ketamine therapy – and it deserves a frank, detailed examination rather than vague reassurances.
IV Ketamine Infusion: The Real Numbers
The cost of a standard IV ketamine induction series – typically six infusions – varies considerably by geography, provider type, and clinic model, but the following ranges reflect current US market conditions:
| Treatment | Typical Cost Range |
|---|---|
| Single IV Ketamine Infusion | $400 – $800 |
| Standard 6-Infusion Induction Series | $2,400 – $8,000 |
| Maintenance Infusion (single session) | $400 – $800 |
| KAP (including therapy fees) | $3,000 – $12,000+ |
| Esketamine (Spravato) per session | $800 – $1,000 (before insurance) |
Major metropolitan areas – New York, Los Angeles, San Francisco, Chicago – tend toward the higher end of these ranges. Smaller markets and telehealth oral ketamine options are typically less expensive, though as discussed, they represent a different treatment entirely.
The Insurance Landscape: Frustrating But Shifting
Here is the honest reality of insurance coverage for ketamine therapy in 2025: it remains deeply inadequate for most patients, though the situation is slowly improving.
IV racemic ketamine infusions for depression are not covered by most major insurance carriers. Because the FDA has not approved IV ketamine for psychiatric indications, insurers classify it as experimental or investigational and routinely deny coverage. Patients pay entirely out of pocket – a financial barrier that disproportionately restricts access for those who may need it most.
Esketamine (Spravato) has a more favorable insurance pathway. As an FDA-approved medication, it is eligible for coverage under many commercial insurance plans and Medicare, though prior authorization is almost universally required. The authorization process typically demands documentation of treatment resistance – evidence that the patient has failed at least two adequate antidepressant trials – along with letters of medical necessity. Even with insurance, patient cost-sharing can be significant, though the manufacturer (Janssen) offers a patient assistance program that substantially reduces out-of-pocket costs for eligible patients.
Strategies for managing cost:
- Clinical trials – The NIH ClinicalTrials.gov database lists ongoing ketamine research studies that may provide free or subsidized treatment in exchange for participation
- Sliding scale clinics – A small but growing number of providers offer income-based pricing for underserved patients
- Healthcare financing – Companies like CareCredit and Prosper Healthcare Lending offer payment plans specifically for medical procedures not covered by insurance
- Employer benefits advocacy – Some patients have successfully advocated for ketamine coverage through their employer’s benefits administrator, particularly with documentation from a treating psychiatrist
- FSA/HSA accounts – Ketamine therapy costs are generally eligible for reimbursement through Flexible Spending Accounts and Health Savings Accounts
The Cost-Benefit Framing That Often Gets Overlooked
When evaluating the cost of ketamine therapy, it is worth placing it in a broader economic context that is frequently absent from the conversation.
A patient who has spent five years cycling through antidepressants – each trial involving prescription costs, psychiatrist visits, the hidden cost of prolonged impaired functioning, lost productivity, and potential hospitalization – has often already spent more, in aggregate, than the cost of a ketamine induction series. This is not a justification for anyone to take on financial hardship they cannot sustain. But it is a reframe worth considering: ketamine therapy’s upfront cost looks different when compared to the cumulative cost of years of treatment that has not worked.
What Are the Risks and Side Effects of Ketamine Therapy?
Any honest discussion of ketamine therapy must include a complete and unvarnished examination of its risks. The treatment’s growing profile has attracted enthusiastic advocates, and enthusiasm – however well-intentioned – can lead to minimization of genuine concerns. Patients deserve better than that.
Short-Term Side Effects During and After Sessions
These are the most common adverse experiences and are typically transient, manageable, and expected when treatment is properly supervised:
- Nausea and vomiting: Among the most frequently reported side effects, particularly in the immediate post-infusion period. Most clinics administer prophylactic anti-nausea medication
- Dizziness and disorientation: Common during the dissociative phase and for a period after the infusion ends; resolves with rest
- Elevated blood pressure and heart rate: A reliable pharmacological effect of ketamine, monitored continuously and generally manageable; of greater concern in patients with pre-existing cardiovascular conditions
- Headache: Reported by some patients in the hours following an infusion
- Fatigue: Many patients feel tired after sessions; this typically resolves after sleep
- Dissociative and perceptual effects: As described in detail in Section 3 – generally the intended therapeutic experience, but occasionally distressing for some patients
Psychological Risks
- Anxiety and psychological distress during sessions: Some patients experience frightening or deeply uncomfortable material during the ketamine experience. Proper screening, preparation, and in-session support significantly reduce this risk but cannot eliminate it entirely
- Post-session mood instability: A minority of patients experience transient worsening of mood or emotional volatility in the days following infusions
- Dissociation outside of sessions: Rare, but some patients report periods of spontaneous dissociative experience between sessions
Long-Term Concerns
Bladder damage – ketamine-induced uropathy – is perhaps the most alarming risk associated with ketamine, but it requires important context. This condition, which can be severe, is associated with chronic, high-frequency recreational ketamine use at doses far exceeding anything used therapeutically. In supervised clinical protocols with standard dosing and frequency, bladder complications are extremely rare. Patients with pre-existing urological conditions warrant extra caution and monitoring.
Cognitive effects: Some patients report transient difficulties with memory and concentration following ketamine sessions. The long-term cognitive implications of repeated therapeutic ketamine administration are an active area of research, and current evidence does not suggest significant lasting impairment at standard clinical doses – but this area merits ongoing surveillance.
The Risk of Psychological Dependence
This is a genuinely nuanced area. Ketamine has abuse potential – it is a Schedule III controlled substance for a reason. In recreational contexts, psychological dependence is well-documented.
In clinical therapeutic contexts, the risk profile is substantially different. The structured, supervised, infrequent administration of therapeutic ketamine is categorically unlike recreational use patterns. However, patients with personal or family histories of substance use disorders warrant careful screening, close monitoring, and – where appropriate – additional safeguards in treatment protocols.
The goal of ketamine therapy is to reduce the need for ongoing treatment over time, not to create indefinite dependence. Providers who encourage escalating frequency of maintenance sessions without clear clinical justification should be questioned.
How Clinical Supervision Transforms the Risk Profile
It bears repeating clearly: virtually every serious risk associated with ketamine is dramatically reduced in a properly supervised clinical setting compared to unsupervised use. The risks enumerated above are real – but they exist in a specific context. Cardiovascular monitoring catches blood pressure elevations. Anti-nausea medication prevents the most common side effect. Trained staff manage psychological distress in real time. Strict protocols prevent the frequency and dose escalation associated with bladder damage.
The risk profile of ketamine in a reputable clinic is not the same as the risk profile of ketamine at a party. These are meaningfully, substantively different things – and conflating them serves no one’s interests.
Knowing who ketamine therapy can help, who it cannot help, what it realistically costs, and what its genuine risks look like gives you the foundation you need to have an informed, honest conversation with a qualified medical professional about whether this treatment belongs in your own story. But having that foundation is not the same as knowing how to act on it. In the final section of this guide, we turn to the questions that bring everything together: how do you actually decide whether to explore ketamine therapy? What questions should you ask a provider? Where is this field heading over the next five years? And what do you do – right now, today – if you think this might be relevant to you or someone you love?
How to Know If Ketamine Therapy Is Worth Exploring
Everything covered in this guide – the neuroscience, the history, the patient experience, the costs, the risks, the conditions it treats – ultimately converges on a single, deeply personal question: is this something I should actually pursue?
That question deserves a thoughtful, structured answer. Not a sales pitch. Not a dismissal. A genuine framework for thinking it through.
The Decision Framework: Starting With the Right Questions
Before picking up the phone to call a ketamine clinic, the most useful thing you can do is sit with a set of honest, clarifying questions. These are not gatekeeping criteria – they are thinking tools. They help you arrive at your conversation with a physician already knowing what you need to communicate and what you need to ask.
Questions to ask yourself first:
- Have you tried at least two antidepressants at adequate doses for adequate durations without achieving meaningful, sustained relief? This is the clinical threshold that typically defines treatment-resistant depression – the primary indication for ketamine therapy
- Is your depression, PTSD, or anxiety significantly impairing your daily functioning – work, relationships, self-care – despite ongoing treatment efforts?
- Have you had a thorough psychiatric evaluation that has ruled out conditions that might change the treatment calculus – such as bipolar disorder, active psychosis, or personality disorders that might complicate the picture?
- Are you currently working with a psychiatrist or mental health professional who is aware of and can coordinate around a ketamine trial?
- Do you have the practical infrastructure in place – financial resources or financing options, a support person to accompany you to sessions, time for the induction series – to pursue treatment properly rather than partially?
- Are you approaching ketamine therapy with realistic expectations – understanding it as a tool that may provide relief and create a window of neuroplasticity to be leveraged, not a permanent cure that requires nothing further?
If your answers to most of these questions point toward genuine candidacy, the next step is a conversation with your doctor – not a ketamine clinic intake form.
The Right First Step: Your Existing Mental Health Provider
This point is made deliberately, because the marketing ecosystem around ketamine therapy has made it easier than ever to bypass the medical relationship that should anchor this decision.
Your psychiatrist or primary care physician should be your first call. Not because ketamine clinics are inherently untrustworthy – many are excellent – but because the decision to pursue ketamine therapy is most safely and most effectively made within the context of a provider who knows your full history, your current medications, your risk factors, and your treatment trajectory.
Bring this guide, or a summary of it, to that conversation if it helps. Clinicians who are unfamiliar with ketamine therapy’s current evidence base – and some older practitioners are – may benefit from being directed toward the published literature. The American Society of Ketamine Physicians, Psychotherapists & Practitioners (ASKP3) publishes clinical guidelines and provider resources that can support that conversation.
If your current provider is dismissive without engaging substantively with the evidence, seeking a second opinion from a psychiatrist with specific expertise in treatment-resistant depression is entirely reasonable.
Questions to Ask a Ketamine Provider Before Committing
Once you have your physician’s input and are evaluating specific providers, the following questions will help you distinguish reputable, rigorously run practices from those operating below the standard of care:
About clinical qualifications and oversight:
- Who are the supervising physicians, and what are their specific credentials and training in ketamine therapy?
- Will a physician be present during my infusions, or available on-site?
- What is your protocol if I experience significant distress or an adverse cardiovascular event during a session?
About the treatment protocol:
- What is your standard induction protocol, and how do you individualize dosing?
- Do you offer integration therapy or can you refer me to an integration therapist?
- How do you monitor and evaluate my response across the induction series?
- What are your criteria for recommending maintenance infusions?
About transparency and informed consent:
- Can you provide written documentation of the risks, benefits, and alternatives before I commit to treatment?
- What is your refund or discontinuation policy if I need to stop treatment partway through?
- Will you communicate with my existing psychiatrist or prescribing physician?
About cost and logistics:
- What is the full cost of the induction series, including any additional fees not listed in your initial pricing?
- Do you offer any financing options or sliding scale pricing?
- What do I need to arrange for transportation, and what are your post-session monitoring requirements?
A provider who answers these questions with patience, transparency, and clinical specificity is demonstrating the kind of professionalism this treatment requires. Vague, evasive, or dismissive responses to reasonable questions are information – and not the good kind.
What Realistic Expectations Actually Look Like
Ketamine therapy is best understood not as a miracle cure, but as a powerful tool – one that can create the conditions for change, but not substitute for the work of living inside that change.
The enthusiasm surrounding ketamine therapy is justified by genuine evidence. But enthusiasm, left unchecked, can set patients up for disappointment that undermines both their experience of the treatment and their broader mental health trajectory.
Here is what the evidence actually supports, stated plainly:
- Ketamine therapy is not a cure. It is a powerful intervention that can produce rapid, meaningful symptom relief – but depression, PTSD, and anxiety are complex, multifactorial conditions that typically require ongoing management
- Response is not universal. Approximately 50–70% of TRD patients show meaningful response to a ketamine induction series – which means 30–50% do not. Non-response is not a moral failure; it is a clinical reality
- Effects are not always permanent. Many patients experience symptom return weeks to months after an induction series and require maintenance infusions and/or ongoing psychotherapy to sustain benefits
- Ketamine works best as part of a broader treatment ecosystem – not as a standalone solution. Patients who combine ketamine treatment with psychotherapy, lifestyle modifications, and ongoing psychiatric care consistently report better long-term outcomes than those who treat it as an isolated intervention
- The experience itself can be challenging. Not every session will feel profound or peaceful. Some will be uncomfortable. Commitment to the full protocol – including integration work – matters enormously to outcomes
Holding these realities clearly does not diminish ketamine therapy’s significance. It makes the decision to pursue it – and the experience of undergoing it – more grounded, more informed, and ultimately more likely to be genuinely transformative.
The Future of Ketamine Therapy – Where Is This Field Heading?
The current state of ketamine therapy is not its final form. The field is evolving rapidly – clinically, scientifically, and politically – and understanding where it is heading helps contextualize its current limitations as temporary rather than permanent.
Expanding Formulations and Delivery Methods
The IV infusion model, while clinically robust, is expensive, time-intensive, and geographically restricted. Researchers and pharmaceutical companies are actively developing and evaluating alternatives:
- Oral and sublingual ketamine – already in use through telehealth platforms, and the subject of ongoing formal trials evaluating efficacy and appropriate protocols for at-home use
- Intranasal racemic ketamine – distinct from Spravato (esketamine), with emerging trial data suggesting potential as a lower-cost, more accessible alternative to IV infusion
- Extended-release and depot formulations – designed to produce sustained, stable ketamine levels rather than the acute peak-and-trough pattern of infusion therapy, potentially extending the duration of antidepressant effects
- Metabolite-based approaches – research into ketamine’s active metabolites – particularly hydroxynorketamine (HNK) – has revealed compounds that may produce antidepressant effects without the dissociative experience, potentially offering the neurobiological benefits with a reduced altered-consciousness profile
The Psychedelic-Assisted Therapy Convergence
Ketamine therapy does not exist in isolation. It is part of a broader, accelerating movement toward psychedelic-assisted psychiatric treatment that represents one of the most significant shifts in mental health research in a generation.
MDMA-assisted therapy for PTSD and psilocybin-assisted therapy for depression and addiction are both in advanced clinical trial stages, with FDA decisions anticipated in the coming years. LSD, ibogaine, and 5-MeO-DMT are subjects of earlier-stage research with compelling preliminary signals.
Ketamine occupies a unique position in this landscape: it is the only currently legal, widely available psychedelic-adjacent treatment in routine clinical use in the US. For many patients and clinicians, it represents a gateway – not to drug use, but to a framework for understanding how non-ordinary states of consciousness can be therapeutically leveraged. The clinical infrastructure, therapeutic models, and regulatory pathways being developed around ketamine therapy are actively informing the broader psychedelic medicine field.
As this convergence matures, the integration of ketamine into a richer, more diverse ecosystem of consciousness-based psychiatric treatment seems increasingly likely – and increasingly well-supported by evidence.
Insurance Coverage Expansion: Legislative Momentum
The insurance access gap for IV ketamine therapy is a genuine equity issue, and it is not going unaddressed. Patient advocacy organizations, professional medical societies, and a growing number of legislators are pushing for expanded coverage, with several specific developments worth watching:
- State-level insurance mandates – several US states have introduced or are considering legislation requiring coverage of ketamine therapy for treatment-resistant depression
- CMS evaluation – the Centers for Medicare and Medicaid Services is under increasing pressure to evaluate and potentially cover IV ketamine, which would have cascading effects on commercial insurer behavior
- Employer benefits advocacy – large self-insured employers are increasingly being approached by benefits consultants about the economic case for covering ketamine therapy as a means of reducing the far larger costs associated with untreated or inadequately treated depression
The timeline for meaningful coverage expansion is uncertain – these processes move slowly – but the direction of travel is clear. Within five years, the insurance landscape for ketamine therapy is likely to look meaningfully different from today’s.
Global Adoption and Emerging Markets
Ketamine therapy is not exclusively an American story. Clinical adoption is accelerating globally:
- United Kingdom – the NHS has begun funding esketamine (Spravato) for treatment-resistant depression in certain regions, and private ketamine clinics have expanded significantly
- Australia – the Therapeutic Goods Administration (TGA) approved esketamine in 2021, and the broader psychedelic medicine framework in Australia is among the most progressive in the world, with psilocybin and MDMA both receiving regulatory approvals in 2023
- Canada – Health Canada has approved esketamine, and ketamine infusion clinics operate in major cities under physician oversight
- UAE and Gulf region – regulatory frameworks for novel psychiatric treatments are evolving, with interest from both healthcare providers and patients in the region growing steadily
- India, Southeast Asia, and Latin America – earlier stage adoption, but with growing awareness and interest among psychiatric communities
The global trajectory reflects a broad shift in how psychiatric medicine is thinking about consciousness, neuroplasticity, and the limits of conventional pharmacology.
AI-Personalized Dosing and Therapy Protocols
Perhaps the most intriguing near-future development in ketamine therapy is the potential application of artificial intelligence to treatment personalization.
Current ketamine protocols are relatively standardized – weight-based dosing, fixed session frequency, uniform induction series structure. But individual variation in ketamine response is substantial, and the factors driving that variation – neurobiological, genetic, psychological, contextual – are complex and difficult to assess manually.
Emerging research is exploring:
- Predictive biomarkers – EEG signatures, genetic markers, and neuroimaging patterns that may predict ketamine response and help identify optimal candidates before treatment begins
- AI-optimized dosing algorithms – machine learning models trained on treatment response data that can individualize dosing recommendations based on real-time patient parameters
- Digital integration platforms – apps and digital therapeutics designed to support the integration process between sessions, track mood trajectories, and flag early signs of response fading that might indicate the need for a maintenance session
These developments are not fully realized yet. But the direction is toward a future where ketamine therapy is less one-size-fits-all and more precisely tailored to the individual – which is likely to improve both response rates and durability of outcomes.
Frequently Asked Questions About Ketamine Therapy
Final Thoughts: A Treatment Worth Taking Seriously
Let’s be clear about what this guide has and has not argued.
It has not argued that ketamine therapy is a miracle cure, that it is right for everyone, or that the enthusiasm surrounding it should be accepted uncritically. The risks are real. The costs are significant. The evidence base, while genuinely compelling, is still maturing in several important areas. And the variability in provider quality demands that prospective patients approach the landscape with informed skepticism rather than blind faith.
What this guide has argued – and what the evidence supports – is that ketamine therapy represents a genuine, clinically validated, and increasingly accessible advance in the treatment of conditions that have caused enormous suffering precisely because they have been so difficult to treat. For a specific population of patients – those with treatment-resistant depression, PTSD, and related conditions – it offers something that the preceding generation of treatments often could not: real relief, arriving quickly, through a mechanism that works when other mechanisms have failed.
That matters. Profoundly.
If you or someone you love has spent years cycling through medications, therapists, and treatment protocols without finding sustainable relief, the conversation about ketamine therapy is worth having – with your doctor, with appropriate caution, and with realistic but genuinely hopeful expectations.
The brain can change. The evidence says so. And for many people, ketamine therapy is part of how that change begins.
This guide was written for informational and educational purposes only. It does not constitute medical advice, and nothing in it should be interpreted as a recommendation to pursue, alter, or discontinue any medical treatment. Always consult a qualified physician or mental health professional before making decisions about your care.

{kind=link}